
Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 1
Medicaid Expansion and the Louisiana Economy
Prepared for
Louisiana Department of Health*
Prepared by
James A. Richardson
Jared J. Llorens
Roy L. Heidelberg
All Professors in the Public Administration Institute at Louisiana State University
March 2018
*This study was funded by a grant from the Louisiana Department of Health in conjunction with the LSU Health
Science Center.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 2
Executive Summary
Medicaid Expansion and the Louisiana Economy
Medicaid expansion provides health insurance for non-elderly adults with income less than 138%
of the Federal Poverty Level. It provides for a 97.5% federal contribution for state fiscal year 2017,
a 94% federal contribution in calendar year 2018, a 93% federal contribution in calendar year
2019, and a 90% federal contribution from calendar year 2020 and beyond, assuming no further
changes in Medicaid at the federal level. This large federal contribution represents an infusion
of federal spending in Louisiana that would not have occurred if the state had not accepted
Medicaid expansion as created in the Patient Responsibility and Affordable Care Act passed by
the U.S. Congress in 2010. This federal infusion creates and sustains economic activity in the
healthcare sector which then impacts all other sectors of the state’s economy.
The economic impact as summarized by the Kaiser Family Foundation is as follows:
Illustration 1. Flow of Medicaid Dollars through Louisiana Economy
State Medicaid Expansion: Policy Decision of State
Leads to
Federal Medicaid Dollars: Net New Dollars to Louisiana Economy (dollars that would not be
present in Louisiana economy if not for Medicaid Expansion)
Providing net new direct
spending for
Healthcare Providers
leads to spending by Healthcare Providers for
Healthcare Vendors and
Healthcare Services
Income Earned by
Employees of Healthcare
Providers
Other Products
and Services
With this spending fostering additional spending in local economy
Consumer Purchases
Business Purchases
Business Investment
All of this activity leads to economic impact on local economy
Business
Transactions
Personal Earnings
Jobs
State and Local Tax
Receipts

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 3
The economic model above has been used by multiple states to evaluate the impact of the
injection of federal dollars for Medicaid programs, including Medicaid expansion:
• The University of Michigan’s Institute for Healthcare Policy & Innovation noted that
Michigan’s expansion of Medicaid health insurance had boosted the state’s economy and
budget and would continue to do so for at least five years.
• Regional Economic Analysis prepared a study for the state of Arkansas and found that
Medicaid expansion in Arkansas had contributed a 0.41% increase in gross domestic
product as of 2014 and would have a continuing positive impact on the growth of GDP
and on state employment through 2020
• The Colorado Health Foundation prepared a report title “Assessing the Economic and
Budgetary Impact of Medicaid Expansion in Colorado: FY 2015-16 through FY 2034-35” in
which they concluded that Medicaid expansion is and will continue to have a significant
positive impact on the state’s economy
• The Commonwealth of Kentucky retained Deloitte Development, LLC to prepare a study
outlining the impact of Medicaid expansion on the state’s economy, with the following
result: the net difference between expanding Medicaid and not expanding Medicaid was
estimated to be a positive $919.1 million from FY 2014 through FY 2021
• “The Real Impact of Medicaid Expansion in Maine,” estimated that expanding Medicaid
coverage in Maine would create 6,000 net new jobs, 4,000 in the healthcare sector and
2,000 in other sectors of the economy.
• A study by the Pennsylvania Department of Human Services (January 27, 2017) found that
the expansion of Medicaid led to an increase of employment by 15,500 jobs and an
increase in state tax revenues of $53.4 million.
• Study by Bureau of Business and Economic Research at the University of Montana
estimated Medicaid expansion created and supported about 5,000 jobs with increases in
personal income of $280 million with about 2,000 jobs being in the healthcare industry
and the other 3,000 jobs scattered in retail, personal services, construction, and the
hospitality industry.
The direct economic impact of Louisiana’s decision to expand Medicaid , based on the type of
healthcare treatment being provided, is illustrated in Table ES.1 for FY 2017. In State Fiscal Year
Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 4
2017, the federal government had an average FMAP of 97.5% for the Medicaid expansion
program, meaning for every dollar the state spent on Medicaid expansion, the federal
government paid 97.50 cents. Louisiana’s choice to participate in the Medicaid expansion
represents an injection of federal dollars into the Louisiana economy that otherwise would not
be present. This means that Medicaid expansion, in addition to providing healthcare for non-
elderly adults with income being less than 138% of the federal poverty level, also creates an
economic stimulus to the state’s economy. In SFY 2017 the net new federal infusion of dollars
amounted to $1.85 billion after adjusting for non-elderly adults being transferred from other
Medicaid programs with lower FMAP rates. This economic impact means sustaining and creating
employment impacts, personal earnings, and state and local tax receipts.
The federal injection of just $1.85 billion created and supported almost 19,200 jobs, state tax
receipts of just over $103 million, and local tax receipts of $74.6 million.
Table ES 1. Economic Impact of Medicaid Expansion Program on Louisiana Economy Based on
Payments to Managed Care Organizations, State Fiscal Year 2017 (in millions)
Type of
Activity
Federal
Payment
Business
Activity
Personal
Earnings
Employment
State Tax
Receipts
Local
Tax
Receipts
Hospitals:
Inpatient Care
$495.5
$939.9
$350.4
5,311
$29.1
$21.0
Outpatient
Care
$297.8
$564.8
$210.2
2,593
$17.5
$12.6
Pharmacy
$284.5
$539.7
$201.2
3,825
$16.7
$12.1
Physicians and
other
Professions
$441.1
$836.5
$311.9
4,420
$25.9
$18.7
Other Medical
Services
$64.6
$122.4
$41.6
1,150
$3.4
$2.5
Administration
of Program
$266.5
$476.8
$124.8
1,818
$10.4
$7.5
Total Activity
of Medicaid
Expansion
$1,850.0
$3,480.1
$1,118.2
19,195
$103.2
$74.6
The infusion of Medicaid expansion federal dollars enhances economic activity and employment
throughout the state as illustrated in Table ES.2. Healthcare activity is a statewide activity so any
increase in a federal infusion of healthcare dollars will be spent throughout the state and will
affect employment and economic activity throughout the state in addition to providing

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 5
healthcare for the state’s citizens. The impact on the various regions of the state as defined by
Health Districts in Map ES.1 is included in Figure ES.1 for FY 2017.
Figure ES.1 Employment Related to Medicaid Expansion
Spending in Health Districts and % of Total Employment, SFY 2017
Map ES.1, Louisiana Health Districts
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
-
500
1,000
1,500
2,000
2,500
3,000
District
1
District
2
District
3
District
4
District
5
District
6
District
7
District
8
District
9
District
10
Employment Related to Medicaid Expansion Program
% of Total Employment in Region

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 6
This economic stimulus will continue as long as the state allows for expanded Medicaid access
under the Affordable Care Act. In addition, there are several important comparisons to note:
(1) The estimated state tax receipts that were generated by the infusion of federal dollars
exceeded the dollars budgeted for the Medicaid expansion program by close to $50
million. This does not include any net budgetary savings from moving participants
from one Medicaid program to Medicaid expansion under a higher FMAP,
(2) The employment support is very important to the state since other sectors of the
state’s economy, such as the oil and gas sector, have been downsizing in Louisiana
since 2014 due to global market conditions
(3) The economic impact associated with the Medicaid expansion program is spread
across the state, and
(4) Any resurgence in the Louisiana economy because of global and national markets or
because of efforts by the state will not be deterred by expansion in the healthcare
industry given the variation in employment training and background.
Last, these economic gains are in addition to the broader gains from people having appropriate
healthcare throughout their adult life. Improved healthcare access can also have a positive effect
the labor force participation rate, defined as the number of persons in the work force who are
16 years of age and older. Improved labor force participation rates should be one long-term
result of the Medicaid expansion program, and rising labor force participation rates will allow for
further employment growth in the state.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 7
Medicaid Expansion and Louisiana Fiscal Outcomes
Introduction: Medicaid and Medicaid Expansion
Medicaid provides, as of 2018, health and long-term care to approximately 1.7 million low-
income children, pregnant women, adults, seniors, and people with disabilities in Louisiana.
Hospitals and nursing homes receive a large share of their funding from Medicaid
reimbursements. Medicaid is a means-tested entitlement program that finances the delivery of
primary and acute medical services as well as long-term services that is jointly funded by the
federal government, through the Federal Medical Assistance Percentage (FMAP), and state
governments.
1
The federal government provides at least 50% of Medicaid funding for every state
and provides more funding for a state according to the state’s FMAP, a formula based on the
average per capita income for each state relative to the national average.
2
In Louisiana, for FY 2018, the FMAP for the long-standing Medicaid program that covers poor,
elderly, and disabled citizens is projected to be 63.90% and 97.58% for the enhanced FMAP or
the Medicaid program for children.
3
In 2012, these FMAPs were 61.09% and 72.76% respectively.
In 2018 the state of Louisiana receives from the federal government 63.90 cents for every dollar
the state spends on healthcare for those individuals covered by Medicaid prior to the expansion
of coverage to poor non-elderly adults under the Affordable Care Act. In FY 2018, Louisiana will
receive 97.58 cents for every dollar it puts into the children’s insurance program so the state pays
on net 2.42 cents per healthcare expenditure for each dollar spent on eligible children. In both
cases of Medicaid coverage, the federal government makes a major contribution to the state’s
overall system of healthcare and related healthcare spending. In 2015, the FMAP for Louisiana’s
LAChip program was 73.44 cents. It was increased to 96.55 cents per dollar in 2016; 96.60 cents
per dollar in 2017; and, now in 2018 it is 97.58 cents per dollar. This higher rate will continue
through 2019 for the enhanced Medicaid program for children.
4
In 2015, prior to Medicaid expansion in Louisiana, almost one half of the population of Louisiana
was insured through employer-supported-insurance plans. Thirteen percent of the population
was insured through Medicare and 21% through Medicaid, two programs initiated and supported
by the federal government with the federal government bearing all of the cost for Medicare and
1
Section 1095 (b) of the Social Security Act specifies the basic formula for calculating the FMAP but with adjustments
as specified by law such as section 614 of the Children’s Health Insurance Program Reauthorization Act of 2009. U.S.
Department of Health & Human Services, Office of the Assistant Secretary for Planning and Evaluation.
2
Medicaid’s Federal Medical Assistance Percentage (FMAP), Alison Mitchell, Congressional Research Service,
February 9, 2016.
3
The enhanced FMAP is the Medicaid program for children.
4
The Affordable Care Act (P.L. 111-148)

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 8
the state and federal government sharing the cost for Medicaid. Seven percent of state residents
were insured privately but not through an employer and 11% of the population, or over 500,000
persons, were uninsured (see Figure 1).
Louisiana’s healthcare distribution is not substantially different from national distribution
averages. For the entire country, 49% of the population had employer-supported-insurance; 14%
had Medicare; 20% had Medicaid; 7% had a non-group insurance plan; and 9% had no insurance.
Figure 1. Source of Healthcare for Louisiana Citizens, Pre Medicaid-Expansion
Source: Medicaid in Louisiana, The Henry J. Kaiser Family Foundation, June 2017.
In 2016, 40% of Louisiana’s population had income less than 200% of the federal poverty level,
the definition of low income, as compared to 30% of the U.S. population.
5
Only two states had a
higher percentage of its population with income less than 200% of the federal poverty level,
Mississippi (42%) and New Mexico (41%). Louisiana’s poverty rate is an important factor in
determining eligibility for Medicaid as well as the federal assistance in paying for the Medicaid
program.
As of 2018, Medicaid plays a major role in both the U.S. healthcare system and in the Louisiana
healthcare system. According to the Henry J. Kaiser Family Foundation,
6
Medicaid accounts for
one-sixth of the dollars spent on healthcare in Louisiana; one-third of dollars distributed to
safety-net hospitals; and half of dollars spent on long-term care. Total healthcare spending in the
state is significant since, according to the Louisiana Workforce Commission, the Healthcare and
5
Distribution of the Total Population by Federal Poverty Level, www.KFF.org. the Henry J. Kaiser Family Foundation.
6
Medicaid in Louisiana, Henry J. Kaiser Family Foundation, June 2017.
48%
13%
21%
7%
11%
Employer Supported
Insurance
Medicare
Medicaid/LAChip
Non-Group
Uninsured

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 9
Social Assistance business sector makes up 16% of total employment and just over 15% of total
payroll in the state.
7
Certain segments of the healthcare industry, the ambulatory healthcare
services and hospitals, each make up 5.5% of total employment in the state and over 6% of the
state’s total payroll.
To provide a context for the state impact of Medicaid expansion under the ACA, the percentage
of uninsured non-elderly adults in the state for 2013 is illustrated in Map 1.
8
As can be seen, rates
varied across the state with northeastern Louisiana having a large number of parishes with the
uninsured rate among non-elderly adults being greater than 25.1%. Large population zones such
as Orleans Parish, East Baton Rouge Parish, Calcasieu Parish, Rapides Parish, Caddo Parish, and
Ouachita Parish had uninsured rates between 19.1% to 25.0%. A quarter of the parishes had
uninsured rates below 19.0%. The uninsured rate for non-elderly adults is much higher than the
uninsured rate among other categories of the population. Overall, Louisiana’s uninsured non-
elderly adults amounted to 22% of non-elderly adults. Prior to Medicaid expansion, uninsured
non-elderly adults lacked access to healthcare apart from emergency services.
7
Louisiana Workforce Commission, Employment and Wages, 2
nd
Quarter 2017.
8
Louisiana Health Insurance Survey, 2013, Division of Economic Development, E. J. Ourso College of Business,
LSU, published in August, 2014.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 10
Map 1. Range of Uninsured Rates in Louisiana by Parish for 19 to 64 years of age
The percent and number of uninsured persons in various categories of non-elderly adults for
2013 is illustrated in Table 1, along with their corresponding income categories. In 2013, there
were 291,000 non-elderly adults that had incomes less than 138% of the FPL. There were 555,285
non-elderly adults without insurance that had incomes up to 400% of the FPL. These estimates
were derived from a survey research project conducted by the LSU Economic Policy Research
Group on behalf of the Louisiana Department of Health. While based upon a sample of state
residents, the data provide a reasonable estimate of the number of people who had no insurance
and would likely be eligible for coverage under Medicaid expansion. This report also noted that,
based on its survey, there were an estimated 404,143 non-elderly adults with income being less
than 200% of the FPL without healthcare insurance or about two-thirds of the uninsured non-

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 11
elderly adults.
9
Some of these individuals included in these estimates were covered by Medicaid
through other mechanisms, and under Medicaid expansion, could be provided coverage under a
more favorable FMAP rate.
Table 1. Uninsured Non-elderly Adults in Relation to Federal Poverty Level
Federal Poverty Level (FPL)
Percent of Uninsured Non-
elderly Adults in Each
Income Category
Number of Uninsured Non-
elderly Adults in Each
Income Category
0 to 13% FPL
35.1%
82,249
13% to 100% FPL
39.3%
126,793
100% to 138% FPL
37.2%
81,958
138% to 150% FPL
37.3%
23,628
150% to 200% FPL
30.9%
89,515
200% to 250% FPL
23.5%
56,641
250% to 300% FPL
20.1%
43,566
300% to 400% FPL
13.8%
50,935
Source: Louisiana Health Insurance Survey, 2013, Division of Economic Development, E. J. Ourso College of
Business, LSU, published in 2014.
A further comparison of Medicaid in the U.S. and Medicaid in Louisiana is provided in Table 2
based on 2015 characteristics. Louisiana had fewer adults receiving Medicaid assistance and
fewer low-income individuals receiving Medicaid assistance than the national average despite
the fact that the share of the population in Louisiana that is low-income exceeds the national
rate. In 2015 Louisiana had not expanded Medicaid coverage to all non-elderly adults with
income below 138% of the federal poverty level (FPL). Instead, Louisiana had utilized a safety-net
healthcare system for its low income non-elderly adults who could not afford healthcare
insurance or who did not fit into another category that was covered by Medicaid.
10
Medicaid
expansion has switched the state from a safety-net model to an insurance model for most of its
lower income citizens. The insurance model could also create substantial health benefits over
time and lower healthcare costs over time given the ability of these non-elderly adults to receive
healthcare prior to emergencies.
9
Louisiana’s Uninsured Population: A Report from the 2013 Louisiana Health Insurance Survey, sponsored by the
Louisiana Department of Health & Hospitals and conducted by the LSU Division of Economic Development and the
LSU Public Policy Research Lab.
10
Louisiana has supported a state-wide charity hospital system since the initiation of the Charity Hospital in New
Orleans in 1732. The charity hospitals were state facilities. The Jindal Administration changed almost all of the
charity hospitals from state facilities to private facilities through contracts between the state and private hospitals.
The state still has a charity hospital system with private hospitals working in the role as charity hospitals for the
state.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 12
Louisiana had a larger number of persons receiving nursing home assistance than the national
average and Medicaid-provided nursing home assistance is covered in Louisiana. Louisiana had
the same number of children and the same number of persons with disabilities using Medicaid
as the national average, again Medicaid programs that have been fully adopted by Louisiana. The
insurance model had applied to all segments of the population except for non-elderly adults.
Table 2. U.S. and LA Comparison with respect to Individuals Using Medicaid, 2015(?)
U.S.
LA
Adults
1 in 7
1 in 8
low-income individuals
1 in 2
2 in 5
Children
2 in 5
2 in 5
Nursing Home Residents
3 in 5
3 in 4
People with Disabilities
2 in 5
2 in 5
* Medicaid in Louisiana, Henry J. Kaiser Family Foundation, June 2017.
The Patient Protection and Affordable Care Act (ACA), signed into law on March 23, 2010, was
intended to broadened access to health insurance. As of 2010 almost 50 million persons in the
United States, or about 15% of the population, did not have any form of health insurance. In
2015, an estimated 500,000 Louisiana residents, about 11% of the total population, lacked access
to insurance. This also amounted to 28% of the population between the ages of 18 and 65, given
that elderly adults are covered by Medicare and Medicaid, as needed, and children and parents
are covered by Medicaid, as needed.
11
The uninsured rate for all children in Louisiana is around
4% and the uninsured rate for Medicaid-eligible children is around 5%.
12
This estimate of
uninsured citizens is consistent with the fact that about 20% of non-elderly adults in Louisiana
live in poverty and with the information provided in the 2013 survey by the LSU Division of
Economic Development.
The method of extending coverage to non-elderly adults via the ACA was through graduated tax
credits for people with incomes between 100% and 400% of the federal poverty level (FPL) and
through an expansion of the Medicaid program to include non-elderly adults whose income is
less than 138% of the FPL.
13
The U.S. Supreme Court in a 2012 decision
14
declared that the federal
government could not force states to expand their Medicaid programs to include this group of
11
“The Louisiana Health Care Landscape,” Kaiser Family Foundation, published June 8, 2016. This number is reduced
by the creation of the Greater New Orleans Community Health Connection, a Medicaid pilot program whose mission
is to provide access to primary care for uninsured adults up to 200% of the FPL with this program servicing close to
40,000 persons.
12
Louisiana Department of Health.
13
The FPL for 2018 is $12,140 for family of 1; $16,460 for family of 2; $20,780 for family of 3; $25,100 for family of
4; $29,420 for family of 5; $33,740 for family of 6; $38,060 for family of 7; and, $42,380 for family of 8.
14
National Federation of Independent Business v. Sebelius, 567 U.S. 519 (2012). This decision upheld the power of
the U.S. Congress to enact most provisions of the Patient Protection and Affordable Care Act, but it did limit the
power of Congress to expand the Medicaid program to include non-elderly adults without the consent of the state.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 13
non-elderly adults, which in effect gave states the choice to expand their Medicaid programs. As
of 2018, 33 states, including the District of Columbia, have expanded their Medicaid programs.
In 2016, Louisiana made a decision to join the Medicaid expansion program.
Impact of Medicaid Expansion on the Budget and the Economy
Much of the debate in all states about whether to adopt or not to adopt Medicaid expansion has
focused on budgetary issues, namely, the cost of the program to the state and the ability of the
state to support the program as the Federal Medical Assistance Percentage (FMAP) for non-
elderly adults is gradually reduced from 100% for 2014, 2015, and 2016 to 90% in 2020.
From a purely budgetary perspective, Medicaid expansion can reduce the cost of the state’s
healthcare program through the following mechanisms:
• Movement of eligible non-elderly adult Medicaid recipients
15
from the lower
federal-match rate for the long-established Medicaid programs to the higher
federal-match rate of the Medicaid expansion program. The transfer came from
four programs including Take Charge Plus with a 90% FMAP for SFY 2016, GNOCHC
with a 62.21% FMAP for SFY 2016, Pregnant Women with a FMAP of 62.21 in SFY
2016 and Persons with Disabilities with a 62.21% FMAP for SFY 2016.
• The GNOCHC transfers, as well as the transfer of Pregnant Women and Persons
with Disabilities, saved Louisiana 35.29 cents for every dollar of Medicaid
expenditures in 2017 for former participants
16
and will save the state 31.29 cents
for every dollar of Medicaid expenditures in SFY 2018 and in SFY 2019, 29.29 cents
in SFY 2020, and 29.79 cents in each year beyond FSY 2020.
• The Take Charge Plus program saved Louisiana 3.5 cents for every dollar of
Medicaid expenditures in SFY 2017 and will save the state 3 cents in SFY 2018 and
SFY2019, and 1.5 cents in SFY 2020. After FSY 2020 the Take Charge FMAP will be
the same as the Medicaid expansion FMAP in 2020 at least as it is currently
established.
• Certain hospital supplemental payments have been funded at the lower federal-
match rate but can now be funded at a higher expansion match rate saving the
state approximately from 30 cents per dollar of eligible Medicaid expenditures in
2017 to 26 cents for every dollar of eligible Medicaid expenditures once the
Medicaid expansion federal/state ratio reaches 90/10
15
Louisiana Department of Health
16
And this comment does not include any benefits from better healthcare service since the GNOCHC program
supported relatively limited healthcare services.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 14
• Newly released state prisoners are now eligible for Medicaid insurance under the
Medicaid expansion program
• Collection of additional premium taxes from the managed care organizations
thereby increasing state revenues, and
• Disproportionate share payments to hospitals will decrease as the number of
uninsured decreases.
Some of these budgetary changes are long-term and will continue to contribute to budgetary
savings for the duration of the program. The state’s share of the Medicaid expansion program
will gradually increase to 10%, so the budgetary savings will be reduced over time. If additional
persons are added to the Medicaid rolls, then this will affect the state’s spending on Medicaid. A
more robust federal match rate for Medicaid expansion allows for the budgetary savings. During
the first three years of Medicaid expansion (2014, 2015, and 2016) the federal government
agreed to fund 100% of the cost for non-elderly adults. Gradually, this federal obligation will fall
to 90% by 2020.
In addition to the budgetary implications of the program for the state, the Medicaid expansion
program also serves as an ongoing economic input given the very favorable FMAP. Medicaid
expansion represents an injection of net new federal dollars that would not be forthcoming
unless the Medicaid expansion program were implemented. The Kaiser Family Foundation
summarized the economic impact of Medicaid spending in a state as shown in Illustration 1, with
this model working for both the Medicaid expansion program and the long-established Medicaid
programs.
17
This model is also outlined in a study by the Urban Institute in June 2013.
18
17
The Role of Medicaid in State Economies: A Look at the Research, Executive Summary, Kaiser Family Foundation,
January 2009.
18
Medicaid Expansion Under the ACA: How States Analyze the Fiscal and Economic Trade-offs, Urban Institute,
June 2013,

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 15
Illustration 1. Flow of Medicaid Dollars through Louisiana Economy
State Medicaid Expansion: Policy Decision of State
Leads to
Federal Medicaid Dollars: Net New Dollars to Louisiana Economy (dollars that would not be
present in Louisiana economy if not for Medicaid Expansion)
Providing net new direct
spending for
Healthcare Providers
leads to spending by Healthcare Providers for
Healthcare Vendors and
Healthcare Services
Income Earned by
Employees of Healthcare
Providers
Other Products
and Services Purchased by
Healthcare Providers
With this net new direct spending fostering additional spending in local economy by
Consumer Purchases
Business Purchases
Business Investment
All of this activity leads to economic impact on local economy
Business
Transactions
Personal Earnings
Jobs
State and Local Tax
Receipts
This economic model has been used by multiple states to evaluate the impact of Medicaid
programs on a state’s economy and on the “real” cost of expanding Medicaid coverage. These
studies focus on the economic impact from a state’s perspective, not from a national perspective
with examples of these studies including the following:
• The University of Michigan’s Institute for Healthcare Policy & Innovation published an
article in the New England Journal of Medicine stating that Michigan’s expansion of
Medicaid health insurance had boosted the state’s economy and budget and would
continue to do so for at least five years.
• Regional Economic Analysis prepared a study for the state of Arkansas and found that
Medicaid expansion in Arkansas had contributed a 0.41% increase in gross domestic
product as of 2014 and would have a continuing positive impact on the growth of GDP
and on state employment through 2020 (“Economic Impacts of the Arkansas Private
Option,” August 2015).

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 16
• The Colorado Health Foundation prepared a report title “Assessing the Economic and
Budgetary Impact of Medicaid Expansion in Colorado: FY 2015-16 through FY 2034-35” in
which they concluded that (1) Medicaid expansion is and will continue to have a
significant positive impact on the state’s economy and (2) the combination of federal
funding, the use of a health provider fee paid by hospitals as the source of revenue for
the state’s share of Medicaid expansion, modest savings in other programs, and increased
state tax revenues due to expansion would result in no net cost to Colorado’s General
Fund.
• The Commonwealth of Kentucky retained Deloitte Development, LLC to prepare a study
outlining the impact of Medicaid expansion on the state’s economy, with the following
result: the net difference between expanding Medicaid and not expanding Medicaid was
estimated to be a positive $919.1 million from FY 2014 through FY 2021, with 90% of this
estimate being related to the positive fiscal impact of Medicaid expansion and the other
10% being related to a negative impact on the state’s budget if Medicaid had not been
expanded.
• A study by Dr. Elizabeth Kilbreth, “The Real Impact of Medicaid Expansion in Maine,”
estimated that expanding Medicaid coverage in Maine would create 6,000 net new jobs,
4,000 in the healthcare sector and 2,000 in other sectors of the economy. This study
preceded a vote by the residents of Maine in 2017 to expand Medicaid. This study also
noted that studies in some states had concluded that Medicaid expansion had reduced
state spending or prior state-only programs and increased revenues from the infusion of
net new federal dollars, thereby offsetting the state revenues required to expand
Medicaid.
• A study by the Pennsylvania Department of Human Services (January 27, 2017) found
that the expansion of Medicaid led to an increase of employment by 15,500 jobs and an
increase in state tax revenues of $53.4 million. The methodology used in this analysis of
the impact of an infusion of federal dollars on the state’s economy is based on the model
used by the Kaiser Family Foundation.
• Study by Bureau of Business and Economic Research at the University of Montana for
Montana estimated Medicaid expansion created and supported about 5,000 jobs with
increases in personal income of $280 million with about 2,000 jobs being in the healthcare
industry and the other 3,000 jobs scattered in retail, personal services, construction, and
the hospitality industry and a previous study in 2015 comparing the results of states that
had expanded Medicaid to Montana which, at that time, had not expanded its Medicaid
Program conducted by the Chief Administrative Officer for the Native American Programs
and Population Management Research in Montana.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 17
This analysis of Medicaid expansion in Louisiana focuses on the economic impact from a state’s
perspective, not from a national perspective. This diagram of the flow of federal Medicaid dollars
through the local economies illustrates the fact that the federal dollars are net new dollars
coming to the state that, otherwise, would not. These dollars initiate payments to the healthcare
sector which in turn initiate payments to vendors providing commodities and services to the
healthcare providers and payments to employees of the healthcare providers and payments to
employees of the vendors. This spending by the healthcare providers lead to a second and third
round of spending by its employees and the healthcare vendors and providers of healthcare
services. The impact of the net new dollars from the federal government has a large impact on
the healthcare community and its vendors and employees but also has an impact on grocery
stores, service stations, personal and business services, and state and local governments. These
jobs, wages and earnings, and state and local tax receipts would not exist if the federal dollars
had not been introduced into the state’s economy. And, the federal dollars would not be
forthcoming if the state had not adopted the Medicaid expansion program.
The state must put up dollars to receive the federal dollars, but, in the case of Medicaid
expansion, Louisiana in calendar 2016 did not have to put up any money so the federal
government paid 100% of the Medicaid expansion program; the state in calendar 2017 had to
put up 5 cents to get 95 cents from the federal government; as of calendar 2018 the state has to
put up 6 cents to get 94 cents, as of calendar 2019 the state will have to put up 7 cents to get 93
cents of federal assistance, and as of calendar 2020 Louisiana will have to put up 10 cents in order
to get 90 cents of federal dollars. For state fiscal year 2017 Louisiana had to pay 2.5 cents of each
dollar put into the Medicaid expansion program and the federal government paid 97.5 cents of
each dollar. For state fiscal year 2018 Louisiana will pay approximately 5.5 cents of each dollar
for the Medicaid Expansion program and the federal government will pay 94.5 cents of each
dollar. The FMAP declines to 90% as of calendar 2020 which means that Louisiana will have to
pay its 10% share starting in state fiscal year 2021. In state fiscal year 2020 the state will have six
months of a FMAP of 93% and then six months of a FMAP of 90%.
There is a cost to the state, but there is also the economic feedback of the net new dollars flowing
to the state to support the Medicaid program that will offset partially or possibly fully the state’s
expenses. The state’s contribution to the Medicaid expansion is a direct cost to be incurred by
the state due to the Medicaid expansion program, but the economic impact of the net new
federal dollars, including any increased employment, earnings, and state and local tax receipts,
is also the result of the Medicaid expansion program. An economic impact coincides with any

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 18
program that brings in net new dollars, but in the case of Medicaid expansion, because of the
size of the federal contribution to the federal/state mix, the impact is notable.
19
This ripple effect is associated with all Medicaid programs since the federal government provides
dollars for healthcare for lower income individuals. These federal Medicaid contributions vary
among programs. In Louisiana in 2018 the FMAP for the long-standing Medicaid program is
projected to be 63.90 and 97.58 for the enhanced FMAP for children.
20
The FMAP for the
Medicaid expansion is projected to be 90.0 starting in calendar 2020, but in calendar 2018 it will
be 94.0 and in calendar 2019 it will be 93.0. In calendar 2018 the state of Louisiana will receive
from the federal government 63.90 cents of every dollar it puts into its long-standing Medicaid
program so the state pays on net 34.10 cents; 97.58 cents for every dollar the state puts into the
children’s insurance program so the state pays on net 2.42 cents; and, 94 cents for every dollar
in the Medicaid expansion program for newly eligible non-elderly adults so the state pays on net
6 cents and 90.6 cents for every dollar the state uses for childless adults in the pre-ACA expansion
so the state pays on net 9.4 cents. In all of these cases, the federal government makes a
contribution to the state’s healthcare plan, but a very significant federal contribution comes
under the Medicaid expansion program as provided in the ACA. And, in all of these cases, there
is an economic ripple effect that creates jobs, earnings, and state and local tax receipts that,
otherwise, would not have occurred.
Louisiana Department of Health Budget: State and Federal Expenditures
The Louisiana Department of Health’s budget and its budget for Medical Vendor Payments are
illustrated in Table 2 highlighting expenditures from the state and the federal government.
Medical vendor payments are the expenditures paid by the state to medical vendors for services
rendered or to managed care organizations The first thing to notice is that Medical Vendor
Payments make up close to 90% of the total state expenditures as of FY 2017. The second thing
to notice is that federal allocations make up close to 70% of all DH spending as of FY 2018.
19
The Medicaid Expansion dollars will come to the state regardless of what dollars Louisiana citizens may be paying
to the federal government.
20
The enhanced FMAP is the Medicaid program for children.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 19
Table 2. Louisiana Budget for Department of Health and Medical Vendor Payments (MVP) (billions $s)
Fiscal
Year
State Funds*
Federal Funds
All Funds
Fed.
as %
of all
Funds
MVP
as %
of
Total
DH
MVP
DH
MVP
DH
MVP
DH
MVP
FY 2012
$2.82
$1.93
$5.138
$4.703
$7.955
$6.633
64.6%
83.4%
FY 2013
$3.01
$2.18
$5.290
$4.928
$8.303
$7.113
63.7%
85.7%
FY 2014
$3.46
$2.70
$5.261
$4.873
$8.726
$7.577
60.3%
86.8%
FY 2015
$3.66
$2.90
$5.374
$4.960
$9.031
$7.862
59.5%
87.1%
FY 2016
$3.59
$2.85
$5.929
$5.471
$9.517
$8.317
62.3%
87.4%
FY 2017
$3.96
$3.20
$7.929
$7.433
$11.894
$10.636
66.7%
89.4%
FY 2018
$4.07
$9.499
$13.568
70.0%
Source: Executive Budgets for Louisiana, Louisiana Division of Administration and Louisiana Department of Health
*includes State General Funds, Statutory Dedications, Fees and Self-Generated, and Interagency Transfers
**Enacted, FY 2018
Total spending in the Louisiana Department of Health, according to the Executive Budget for the
state, increased in nominal dollars from $8.247 billion in FY 2012 to $13.594 billion in FY 2018.
This increase includes both state and federal revenues. The DH budget increased from FY 2012
to FY 2016 by about $1.3 billion or about $320 million per year. The growth in federal revenues
in DH’s budget from 2012 through 2016 or before Medicaid expansion was 15.4% and the growth
in state spending was 27.4%. This growth corresponded to rising healthcare prices relative to the
overall inflation rate, to a rising population with additional pressure on the state support for
uninsured individuals, and with a slightly improving FMAP for the state so Louisiana picked up
slightly more federal dollars for each Medicaid claim.
In 2016 Louisiana made a decision to become part of the Medicaid expansion program as created
by the ACA in 2010. From 2016 to 2018 the growth in federal spending was 60.2% and the growth
in state spending was 13.4%. This represents a major change in the source of funds for the
support of the Medicaid program and a major expansion of persons now covered by an insurance
network.
This decision expanded the number of persons who could qualify for Medicaid to include non-
elderly adults with an income equal to or below 138% of the federal poverty level. Many of these
people were already being serviced by the state in an emergency management system. That is,
if they became seriously ill, they could go to one of the state’s private hospitals that had been
contracted to provide healthcare service to persons who did not have healthcare insurance. And,
even more significantly, the uninsured who became ill, but not in what would typically be called
an emergency, would also seek service through emergency rooms. Under the pre-2016 system,

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 20
the federal government put up about 64% of the cost of taking care of persons under the
emergency management system. The state still incurred and will continue to incur a cost for
uninsured non-elderly adults even if the state had not accepted Medicaid expansion, but with a
lower degree of federal support.
The federal share of DH’s budget rose from 62.3% in FY 2016 to 66.7% in FY 2017 and is projected
to be 70.0% in FY 2018. This is due to the fact that the federal government subsidizes the
healthcare program for non-elderly adults more generously than for the long-standing Medicaid
programs. This estimate of 70% federal assistance for the state of Louisiana may diminish
modestly since the FMAP for Medicaid expansion will decline from the 94% federal share in 2018
to the 90% federal share in 2020. This estimate of the federal/state ratio also depends on the
proportion of persons on the long-established Medicaid programs and those who are eligible for
the Medicaid expansion program.
The share of federal spending on the Medicaid program is important since these are dollars that,
otherwise, would not come to the Louisiana economy. From FY 2016 to FY 2017 the increase in
federal spending made up 80% of the overall increase in the DH budget, while from FY 2017 to
FY 2018 the federal spending for DH is projected to make up over 100% of the increase in DH
spending so state outlays are projected to decrease.
The source of payments for healthcare is a very important metric given the economic impact of
federal spending as noted in Illustration 1. The increasing role of federal spending in the
healthcare budget is illustrated in Figure 2. Federal support for healthcare spending in Louisiana
grew more rapidly than state spending in FY 2016 and FY 2017 and, as currently projected, in FY
2018. Just over 70% of LDH’s budget comes from the federal government. Based on information
from the House Fiscal Division approximately 24% of the remainder of the state’s budget is
financed by federal funds.
21
21
FY17-18 Executive Budget Review, Louisiana Department of Health, House Committee on Appropriations,
prepared by House Fiscal Division, April 5, 2017.
Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 21
Figure 2. Growth in DH Budget for FY 2013 through FY 2018.
Increases in federal support for the Louisiana Medicaid project will not eliminate the need for
the state to use some of its dollars to support the state’s healthcare program. The state still has
to make decisions regarding how much of its budget to focus on healthcare for lower income
non-elderly adults, but the federal dollars provide another factor in bringing net new dollars to
the state that would not be spent in the state without the state’s investment in healthcare for its
non-elderly citizens.
LDH spending on healthcare is illustrated in Figures 3 and 4 in terms of nominal and real
expenditures from FY 2012 through FY 2018. The purpose of these figures is to give perspective
to the increases in healthcare spending over the last six years. In Figure 3 both nominal and real
expenditures on healthcare have increased from just over $8 billion in 2012 to about $13.8 billion
in nominal terms by FY 2018 and about $11.6 billion in real terms.
22
In Figure 4 real healthcare
expenditures per capita are illustrated with real per capita spending rising from $1,792 in 2012
to $2,447 in 2018. This increase is consistent with the Medicaid expansion program initiated in
2016. Real state healthcare spending per capita increased from $665 in 2012 to $733 in 2018, an
increase of just over 10%. Real federal healthcare spending per capita increased from $1,127 in
2012 to $1,714 in 2018 or an increase of over 52%. Healthcare spending has grown from 2012
through 2018, but this increase has been dominated by federal outlays.
22
Real expenditures are derived by dividing the nominal expenditures by the consumer price index for healthcare
with this index including healthcare commodities and services. The CPI for healthcare has averaged about 70% above
the CPI for all goods and services over the last 20 years based on information from the U.S. Bureau of Labor Statistics.
10.9%
-4.6%
9.0%
0.1%
27.9%
11.7%
6.4%
-4.7%
8.0%
4.3%
35.8%
18.2%
18.5%
-4.4%
10.5%
-6.3%
14.8%
-1.1%
FY13 FY14 FY15 FY16 FY17 FY18
DH Budget, Total Federal Funds for DH State Funds for DH

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 22
Figure 3. Nominal and Real Expenditures in Healthcare in Louisiana, including
Federal and State
Table 2, Figure 2, Figure 3, and Figure 4 highlight the expanding role of the federal government
in the Medicaid program with respect to the source of funding for the program. This increasing
federal role with respect to financing the Medicaid program permits the state to improve its
budgetary status as opposed to not having the Medicaid expansion program and also allows the
state’s economy to be stimulated by a new and larger source of federal dollars that, otherwise,
would not be have been spent in Louisiana. The increasing federal role in supporting healthcare
for non-elderly adults who makes less than 138% of the federal poverty level also enhances
healthcare for a group of people who have had a very high rate of being uninsured.
$6,000,000,000
$7,000,000,000
$8,000,000,000
$9,000,000,000
$10,000,000,000
$11,000,000,000
$12,000,000,000
$13,000,000,000
$14,000,000,000
SFY12 SFY13 SFY14 SFY15 SFY16 SFY17 SFY18
Nominal Real

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 23
Figure 4. Real Healthcare Expenditures per capita (state and federal)
Medicaid and Medicaid Expansion in Louisiana
Medicaid recipients includes the aged, disabled, families and children, and others, all meeting
certain income requirements. The Medicaid enrollees and payments, pre-Medicaid expansion,
are noted in Figure 5 for Louisiana and the United States representing a division of Medicaid
resources among the different eligible categories. Louisiana has relatively more children in its
Medicaid program than the national average and spends slightly more on the children as part of
its total Medicaid expenditures than the national average. But 58% of the Medicaid enrollees in
Louisiana account for only 29% of Medicaid payments. Similarly, 15% of the enrollees in Louisiana
are classified as parents and this group accounts for only 9% of the Medicaid payments. Disabled
Medicaid enrollees in Louisiana make up 18% of the total enrollees but account for 45% of the
Medicaid payments. Louisiana also has a slightly larger number of disabled persons and spends
slightly more on their treatment. Louisiana has 18% of its Medicaid enrollees as disabled
compared to the national average of 15%. Disabilities account for 45% of the Louisiana Medicaid
expenditures compared to the national average of 42%. Louisiana spends less on its parents than
the national average and parents represent a smaller percentage of enrollees in Louisiana than
the national average. In Louisiana a larger share of the expenditures is on children than the
national average. We do not have information presently to say how the Medicaid expansion
enrollment and expenditures will compare. Figure 5 certainly conveys the message that there
can be and there is a significant difference between the enrollees in Medicaid and the percentage
of resources used in the treatment of these enrollees. This is not surprising since it is very
FY 2012 FY 2013 FY 2014 FY 2015 FY 2016 FY 2017 FY 2018
Real Federal Spending per Capita Real State Spending per Capita
Real Healthcare Spending per Capita

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 24
reasonable to expect a disabled patient to cost much more than a young child for medical
treatment or, for that matter, an adult without any disability as compared to a disabled patient.
Figure 5. Medicaid Enrollees and Payments for U.S. and LA,
not including Medicaid Expansion
Enrollment in the Medicaid program after Medicaid expansion is illustrated in Figure 6. Children
and parents make up just over 50% of the total Medicaid enrollees and the non-elderly adults
covered by the Medicaid expansion program now make up just under 29% of the total enrollees.
The aged and disabled make up a small percentage of the enrollees, less than 15%, but will
continue to make up a much larger share of the Medicaid expenditures.
15%
18%
42%
45%
9%
9%
22%
17%
27%
15%
15%
9%
49%
58%
21%
29%
U.S. LOUISIANA U.S. LOUISIANA
ENROLLEES PAYMENTS
Disabled Elderly Parents Children

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 25
Figure 6. Enrollment in Medicaid by Category
Medicaid expansion payments for hospitals, outpatient care, pharmacy payments, physicians and
other professionals, and all other categories of healthcare spending are illustrated in Table 5.
The Medicaid payments include managed care organization fees and fees for services provided
as paid directly by the state. Almost all of the expenditures will be for managed care
organizations. We have divided the Medicaid payments into various types of expenditures since
each of these healthcare expenditures has different impacts on the local economies.
Table 5. Total Payments by Type of Healthcare Expenditure for Medicaid Expansion Program,
FY 2017 (in millions of dollars)
Expenditures
Federal
Contribution
State Share
Total
Expenditures
% of Total
Hospitals
$495.6
$12.7
$508.3
26.8%
Outpatients
$297.8
$7.6
$305.4
16.1%
Pharmacy
$284.5
$7.3
$291.8
15.4%
Physicians and
Professionals
$441.1
$11.3
$452.3
23.8%
All Other
Healthcare
Spending
$64.6
$1.7
$66.3
3.5%
Administration
$266.4
$6.8
$273.2
14.4%
Total
$1,850.0
$47.4
$1,897.4
3.6%
10.7%
50.8%
6.1%
28.9%
aged disabled children and parents Other medicaid expansion

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 26
We can also note that there was a noticeable increase in claim accounts of 51,000,000 in FY 2016
to 66,000,000 in FY 2017.
23
This increase in the claim accounts certainly illustrates the increased
usage of Medicaid and indicates the movement from an emergency service program to a health
insurance program.
The increase in overall Medicaid enrollees from FY 2016 to FY 2017 represented only about one-
third of the total number of Medicaid expansion enrollees which suggest a number of Medicaid
enrollees moved from one enrollment option to the Medicaid expansion enrollment option and
a number of non-elderly adults who had not been on any Medicaid program but are eligible under
the Medicaid expansion guidelines chose to enroll. Non-elderly adults switching from other
Medicaid programs included 222,367 from the Take Charge Plus program, a program for family
planning services; 65,495 from the Greater New Orleans Community Health Connection; and, a
number of persons from the program for pregnant women and for those with disabilities that
would qualify for Medicaid expansion.
The information about Medicaid in Louisiana as of 2018 can be summarized as follows:
• A large number of people have taken advantage of the Medicaid Expansion
program—over 545,000 persons, but this number is much larger than the increase
in total Medicaid enrollees so non-elderly adults who had been on other Medicaid
programs were able to switch to the Medicaid expansion program with a much
more favorable FMAP.
• The increase usage of the Medicaid program is also documented by the increase
in claim accounts from almost 51,000,000 to just over 66,000,000 from FY 2016 to
FY 2017
• The Medicaid expansion program has been successful in terms of soliciting eligible
citizens to sign up for the health insurance program.
• Public programs such as the Medicaid expansion are not free; rather, there is a
financial cost to the state as well as benefits from improving the health of citizens
of the state. In the case of Medicaid expansion, this cost to the state is reduced
by
o The very high FMAP associated with this program so the federal
government has decided to accept a larger share of the cost of the
Medicaid expansion program
23
Louisiana Department of Health.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 27
o Certain non-elderly adults other Medicaid programs have switched to
Medicaid expansion thereby benefiting the state due to the higher FMAP
associated with the Medicaid expansion program
o And the infusion of net new federal dollars into the economy creates an
economic dynamic that leads to net new jobs and earnings and state and
local tax receipts. This is a dynamic factor that should not be overlooked
as the Medicaid expansion program is evaluated.
Hence, appreciating the true cost of the Medicaid expansion program to the state is not as simple
as examining the budget of the program. It must be accompanied by an analysis of the overall
impact including both the budgetary impact and the overall impact of the net new federal dollars
on the state and regional economies.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 28
Economic Impact of Medicaid Expansion Program on Louisiana Economy and on State
Revenues
The process of estimating the economic impact of the Medicaid expansion program includes the
following steps.
1. Keep in mind the economic ripples being generated by the net new dollars being put into
the Louisiana economy as illustrated in Illustration 1. These economic ripples are being
magnified by the FMAP on Medicaid expansion as opposed to other Medicaid programs.
The model is based on the Regional Input-Output Modeling System as developed by the
U.S. Department of Commerce, Bureau of Economic Analysis.
Illustration 1. Flow of Medicaid Dollars through Louisiana Economy
State Medicaid Expansion: Policy Decision of State
Leads to
Federal Medicaid Dollars: Net New Dollars to Louisiana Economy (dollars that would not be
present in Louisiana economy if not for Medicaid Expansion)
Providing net new direct
spending for
Healthcare Providers
leads to spending by Healthcare Providers for
Healthcare Vendors and
Healthcare Services
Income Earned by
Employees of Healthcare
Providers
Other Products
and Services Purchased by
Healthcare Providers
With this net new direct spending fostering additional spending in local economy by
Consumer Purchases
Business Purchases
Business Investment
All of this activity leads to economic impact on local economy
Business
Transactions
Personal Earnings
Jobs
State and Local Tax
Receipts
2. Identify the number of Medicaid enrollees in the Medicaid Expansion program on
statewide basis and by the ten health districts as illustrated in Map 2. These health
districts have as few as 1 parish in District 10 (Jefferson) and 3 parishes in District 1
(Orleans, Plaquemines, and St. Bernard) to 12 parishes in District 8 (Caldwell, East Carroll,
Franklin, Jackson, Lincoln, Madison, Morehouse, Ouachita, Richland, Tensas, Union, and
West Carroll).

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 29
Map 2. Health Districts in Louisiana, Louisiana Department of Health
3. Medicaid enrollees for FY 2017 are noted in Table 5. The total enrollees will include some
double-counting due to a person having changed classifications during the year.
Table 5. Medicaid Enrollees by Type of Eligibility, FY 2017
Aged
Disability
Parents &
Children
Medicaid
Expansion
Others
Total
Enrollees*
%
Medicaid
Expansion
District 1
11,026
27,923
89,734
74,727
26,618
230,028
32.5%
District 2
12,049
28,519
126,424
66,845
28,162
261,999
25.5%
District 3
8,155
20,173
80,071
44,657
21,097
174,153
25.6%
District 4
14,748
29,846
130,158
70,071
29,909
274,732
25.5%
District 5
5,908
12,913
62,120
31,830
14,451
127,222
25.0%
District 6
8,512
18,827
64,732
33,346
16,180
141,597
23.5%
District 7
13,565
32,277
111,843
60,283
26,754
244,722
24.6%
District 8
10,102
21,285
81,914
48,078
20,565
181,944
26.4%
District 9
10,403
22,860
105,870
56,261
26,201
221,595
25.4%
District
10
8,625
18,089
87,270
56,731
20,167
190,882
29.7%
Others
3,117
3,117
100.0%
Louisiana
103,093
232,712
940,136
545,946
230,104
2,064,219
26.4%

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 30
Medicaid enrollees without any double-counting came to 1,791,69 in 2017 as opposed to
the 2,064,219 as noted in Table 5. The enrollees in Table 5 reflect the persons who, at
one time during FY 2017, were classified in a particular program.
4. Approximately 26.4% of Medicaid enrollees are entered in Medicaid expansion in FY 2017
with the largest percentage being in District 1, including Orleans, Plaquemines, and St.
Bernard parishes, with 32.5% of this District’s Medicaid enrollees be in the Medicaid
expansion program and District 10, which is Jefferson Parish, having almost 30% of their
Medicaid enrollees being in Medicaid expansion. Districts 2 through 9 hovers around 25%
of their Medicaid enrollees being in Medicaid expansion.
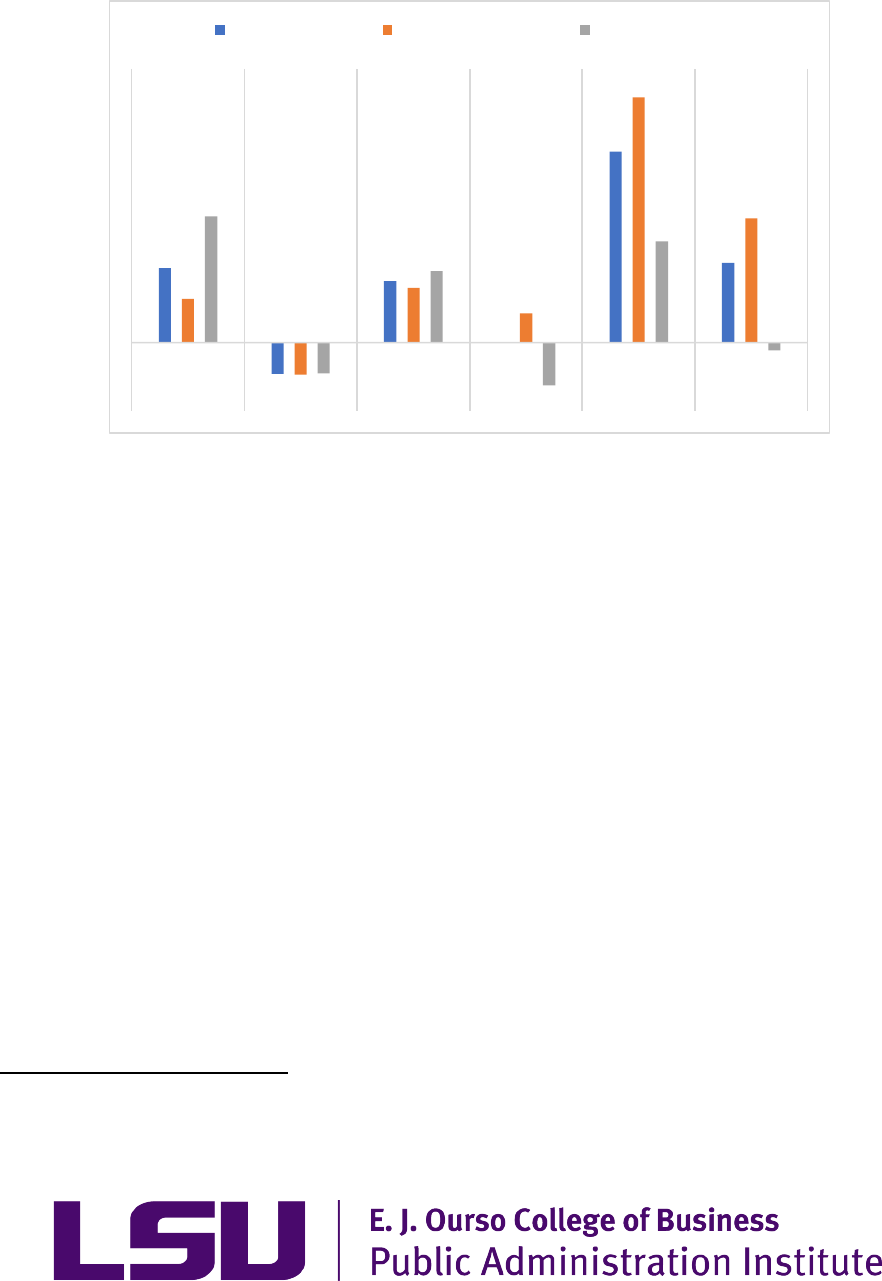
5. Medicaid expansion enrollees and spending are compared to population of each district
in Figure 6. The percentage of Medicaid expansion enrollment and spending exceeds the
population percentage in Districts 1 (New Orleans) , 4 (Lafayette), 7 (Shreveport), 8
(Monroe) and 10 (Jefferson). In Districts 2 (Baton Rouge), 3 (Houma-Thibodaux), and 9
(Northshore) the percentage of Medicaid expansion enrollment and spending is lower
than the percentage of population. In Districts 5 and 6 the percentage of population and
Medicaid expansion enrollment and spending are approximately the same.
Figure 6. Comparison of Population and Medicaid Expansion Enrollment
6. The Medicaid expansion activities of these enrollees in terms of payments for services
received in FY 2017 are illustrated in Table 6 by Districts with these medical activities
being Inpatient Hospital Care, Outpatient services, Pharmacy, Professional Visits
(including visits to Doctors and other medical professions), other medical activities, and
administration. Medicaid expansion expenditures total close to $1.9 billion with $452
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
District
1
District
2
District
3
District
4
District
5
District
6
District
7
District
8
District
9
District
10
% of Medicaid Expansion Enrollment % of Medicaid Expansion Spending
% of Population

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 31
million going to Physicians and professional visits and medical assistance, $291.8 million
being for pharmacy and prescriptions, $508.3 million for inpatient hospitals, $305.4
million for outpatient services, $66.2 million for other healthcare services, and $273.2
million for administration. Districts 1, 2, and 8 tend to spend relatively more Medicaid
expansion expenditures than the percentage of Medicaid expansion enrollees. For
example, Health District 1 has 11.2% of the Medicaid enrollees but spend about 11.5% of
Medicaid expansion expenditures and in District 2 Medicaid enrollees make up about
12.8% of the total Medicaid expansion enrollees but about 13.6% of the Medicaid
expansion estimated expenditures.
Table 6. Medicaid Expenditures by Type of Healthcare Activity for Medicaid Expansion Program
Including both Federal and State Contributions, FY 2017 (in millions)
Medical
Services:
Hospitals
Inpatient
Medical
Services:
Outpatient
and Other
Services
Medical
Services:
Pharmacy
Medical
Services:
Physicians
and Other
Professionals
Other
Medical
Services
Total
District 1
$61.8
$37.7
$45.1
$53.3
$6.7
$204.6
District 2
$78.9
$41.3
$42.0
$53.6
$8.3
$224.2
District 3
$40.6
$28.2
$25.4
$40.0
$6.0
$140.2
District 4
$59.5
$39.6
$36.3
$57.4
$10.2
$202.9
District 5
$33.1
$17.6
$14.4
$24.9
$5.0
$95.1
District 6
$36.6
$20.3
$16.2
$30.7
$5.1
$108.9
District 7
$55.2
$31.1
$25.6
$49.9
$5.9
$167.7
District 8
$43.1
$29.2
$24.7
$47.8
$7.0
$151.7
District 9
$53.1
$35.1
$31.4
$51.1
$7.9
$178.6
District 10
$46.3
$25.3
$30.8
$43.6
$4.2
$150.1
Administration
$0.0
$0.0
$0.0
$0.0
$273.2
$273.2
Total
$508.3
$305.4
$291.8
$452.3
$66.2
$1,897.2
7. The expenditures in Table 6 are state dollars coupled with federal dollars and, in the case
of Medicaid expansion, the federal government in state fiscal year 2017 put up 97.5% of
the total expenditures so for every 2.5 cents the state spent on healthcare for non-elderly
adults with incomes less than 138% of the FPL, the federal government injected 97.5
cents. In FY 2017 the federal government put up $1.85 billion for the state to spend
$1.897 billion so the state’s contribution was less than $50 million. This $1.85 billion
represents new Medicaid expansion enrollees as well as switching non-elderly adults from
other Medicaid programs to the Medicaid expansion program.
24
24
This model accounts for all Medicaid Expansion enrollees regardless of his or her previous enrollment in a Medicaid
program. The model, however, does not allow for any budgetary savings by the state due to the fact that the FMAPs
will be different for Medicaid Expansion as opposed to the previous program in which he or she were enrolled.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 32
The economic impact of the federal input to Medicaid expansion expenditures for state
fiscal year 2017 is illustrated in Table 7 with this economic impact to include overall
business transactions, earnings, employment, and state and local tax collections related
to the federal contribution to the Medicaid expansion program.
Table 7. Economic Impact of Federal Contribution to Medicaid Expansion Program in 2017 (all dollars
in millions)
Type of
Healthcare
Activity
Federal
Payment
Business
Activity
Personal
Earnings
Employment
State Tax
Receipts
Local Tax
Receipts
Hospitals:
Inpatient Care
$495.5
$939.9
$350.4
5,311
$29.1
$21.0
Outpatient
Care
$297.8
$564.8
$210.2
2,593
$17.5
$12.6
Pharmacy
$284.5
$539.7
$201.2
3,825
$16.7
$12.1
Physicians and
other
Professions
$441.1
$836.5
$311.9
4,420
$25.9
$18.7
Other Medical
Services
$64.6
$122.4
$41.6
1,150
$3.4
$2.5
Administration
of Program
$266.5
$476.8
$124.8
1,818
$10.4
$7.5
Total Activity
of Medicaid
Expansion
$1,850.0
$3,480.1
$1,118.2
19,195
$103.2
$74.6
Source: U.S. Department of Commerce, Regional Input-Output Multipliers, based on 2015 Regional Data
The key takeaway from Table 7 is that the economic ripples from the infusion of federal
dollars into the Medicaid expansion program leads to net new state tax receipts being
generated that offsets the state’s expenditures and leaves a net revenue improvement of
$55.7 million of state tax receipts after allowing for the state spending its share of the
Medicaid expansion obligation. In addition, the infusion of federal dollars generates
$74.6 million for local governments.
8. The total economic impact and budgetary affect includes the following parts:
a. Additional Costs to State in state fiscal year 2017: $47.431 million
b. Additional spending by Federal Government in Louisiana: $1.850 billion
c. Gains from the Economic Impact of Federal Spending
i. creating and supporting 19,195 jobs in sectors throughout the economy
and across the state

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 33
ii. creating and supporting personal earnings of $1.118 billion throughout the
economy and across the state
iii. enhancing state revenues by an estimated $103.2 million
iv. enhancing local revenues by an estimated $74.6 million across the state
and political sub-divisions
9. In calendar 2018 the federal government will put up 94% so for state fiscal year the FMAP
will average 94.5%; in calendar 2019 the federal government will put up 93% so the FMAP
for state fiscal year 2019 will average 93.5%; and in 2020 the federal government will put
up 90% so for fiscal year 2020, the FMAP will average 91.5%.
10. The above estimates take into account the transfer of Medicaid enrollees from other
Medicaid programs in which the federal match was less than the 95% match in calendar
2017.
11. The earnings and jobs will not just be in the healthcare sector. About 50% of the jobs will
be in the healthcare sector and the other jobs will be in trade, personal services, food
services, arts and entertainment, and other such sectors that cater to individuals living in
a community.
12. These earnings and jobs are also spread throughout the state as noted in Table 8 which
provides the breakdown of earnings and jobs by district.
Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 34
Table 8. Economic Impact of Medicaid Expansion in Various Regions of the State
(Dollars in millions)
District
Personal Earnings
Employment
Local Tax Receipts
District 1 (New
Orleans)
$141.0
2,202
$8.46
District 2 (Baton
Rouge)
$154.4
2,405
$9.27
District 3 (Houma-
Thibodaux)
$96.5
1,498
$5.79
District 4
(Lafayette)
$139.7
2,183
$8.38
District 5 (Lake
Charles)
$65.4
1,021
$3.93
District 6
(Alexandria)
$75.0
1,162
$4.50
District 7
(Shreveport)
$115.5
1,774
$6.93
District 8 (Monroe)
$104.5
1,618
$6.27
District 9
(Northshore)
$123.0
1,910
$7.38
District 10
(Jefferson)
$103.4
1,605
$6.21
Louisiana
$1,118.6
19,195
$74.60
13. This economic impact will be felt around the state since healthcare is a state-wide activity
as illustrated in Figure 7. Medicaid expansion employment ranges above 2,000 in three
districts (New Orleans, Baton Rouge, and Lafayette); between 1,500 to 2,000 in four
districts (Shreveport, Monroe, Northshore, and Jefferson); and, between 1,000 and 1,500
in three districts (Houma-Thibodaux, Lake Charles, and Alexandria). This employment
related to the Medicaid expansion program represents about 1% of total employment
throughout the state but represents slightly more in Alexandria and Monroe.

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 35
Figure 7. Employment Related to Medicaid Expansion
Spending in Health Districts and % of Total Employment
14. The economic impact of the Medicaid expansion will continue as long as the state
maintains the program and as long as no major changes are instituted by the federal
government, either through acts of the U.S. Congress or regulatory decisions made by the
Center for Medicare & Medicaid Services.
15. This economic and fiscal are already built into the employment and fiscal numbers for
Louisiana.
Summary and Conclusions
Medicaid expansion provides health insurance for non-elderly adults with income less than 138%
of the Federal Poverty Level with a 97.5% federal contribution for state fiscal year 2017, a 94%
federal contribution in calendar year 2018, a 93% federal contribution in calendar year 2019, and
a 90% federal contribution starting in calendar year 2020 and beyond assuming no further
changes in Medicaid at the federal level. This large federal contribution represents an infusion
of federal spending in Louisiana that would not have occurred if the state had not accepted
Medicaid expansion as created in the Patient Responsibility and Affordable Care Act passed by
the U.S. Congress in 2010. This federal infusion creates and sustains economic activity in the
healthcare sector which then spreads over to all other sectors of the state’s economy.
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
-
500
1,000
1,500
2,000
2,500
3,000
District
1
District
2
District
3
District
4
District
5
District
6
District
7
District
8
District
9
District
10
Employment Related to Medicaid Expansion Program
% of Total Employment in Region

Medicaid Expansion and Louisiana Fiscal Outcomes
March 2018
Page 36
This economic stimulus will continue as long as the state continues to provide expanded Medicaid
access and assuming there are no major changes made by the U.S. Congress. There are several
important impacts that the state policy makers should be aware of:
(5) The estimated state tax receipts generated by the infusion of federal dollars exceeded
the state dollars budgeted for the Medicaid expansion program by over $50 million
and this does not include any net budgetary savings from moving participants from
one Medicaid program to Medicaid expansion with the higher FMAP,
(6) The employment support is very important to the state since other sectors of the
state’s economy such as the oil and gas sector has been downsizing in Louisiana since
2014 due to global market conditions
(7) The economic impact associated with the Medicaid expansion program is spread
across the state and will be sustained as long as Medicaid expansion is sustained, and
(8) Any resurgence in the Louisiana economy because of global and national markets or
because of efforts by the state will not be deterred by the expansion in the healthcare
industry given the variation in employment training and background.
These economic gains are in addition to the healthcare gains from people having appropriate
healthcare throughout their adult life. Such healthcare can also positively affect the labor force
participation rate, defined as the number of persons in the work force who are 16 years of age
and older. Improved labor force participation rates should be long-term results of the Medicaid
expansion program. And rising labor force participation rates will allow for further employment
growth in the state.
