
1
Document
history
Publication date
Description of main changes
Version 1
October 2019
Version 2
December 2020
Endorsement by additional Member States (LT, SI)
Version 3
April 2022
Amendment of intended start and end dates (Section 3.1)
Version 4 May 2022
Removal of The Institute of Eye Surgery, UPMC Kildare Hospital
from the application
1
This document has not been adopted by the European Commission and, therefore, it does not contain the official position
of the European Commission.
2
Council Decision 2002/813/EC establishing, pursuant to Directive 2001/18/EC of the European Parliament and of the
Common application form for investigational medicinal products for
human use that contain or consist of AAV vectors
1
Note 1: This application form can be used for submissions in the following jurisdictions: Austria,
Belgium, Croatia, Czech Republic, Denmark, Finland, France, Germany, Hungary, Ireland, Italy, Latvia,
Lithuania, Luxembourg, the Netherlands, Portugal, Romania, Slovenia and Spain.
Note 2: The application form must be accompanied by the SNIF (summary notification information
format for notifications concerning the deliberate release into the environment of genetically
modified organisms for purposes other than for placing on the market)
2
in the case of submissions
that are made under Directive 2001/18/EC.
1
Council, the summary notification information format for notifications concerning the deliberate release into the
environment of genetically modified organisms for purposes other than for placing on the market (OJ L 280,18.10.2002,
p.62).

2
1. Introduction
Clinical trials conducted in the EU with investigational medicinal products that contain or consist of
genetically modified organisms ("GMOs"
3
) must comply with the legislation governing the
authorization of clinical trials.
4
Clinical trials with medicinal products that contain or consist of GMOs must also comply with applicable
requirements under Directive 2001/18/EC on the deliberate release into the environment of
genetically modified organisms
5
("deliberate release framework") and/or under Directive 2009/41/EC
on the contained use of genetically modified micro-organisms ("contained use framework").
6
This application form implements the requirements of the Directive 2009/41/EC and of the Directive
2001/18/EC, as adapted to the specific characteristics of adeno-associated viral vectors (“AAVs”)
contained in investigational medicinal products for human use.
This is an application form for investigational medicinal products for human use that contain or consist
of AAVs (hereafter referred to as “clinical vectors”). However, if the application concerns an
investigational medicinal product that contains or consist of AAVs that has already been granted a
marketing authorisation, the submission form for use in case of clinical trials with authorised medicinal
products should be used (provided that the submission form has been endorsed by the competent
authorities in the relevant jurisdiction).
The application form has been endorsed by Austria, Belgium, Croatia, Czech Republic, Denmark,
Finland, France, Germany, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, the Netherlands,
Portugal, Romania, Slovenia and Spain.
2. Explanatory notes
The common application form is without prejudice to consultation requirements that exist under
Directive 2001/18/EC.
In addition, certain national requirements may need to be considered by developers of medicinal
products before they submit the application form to the relevant competent authorities:
3
Throughout this document, the term “GMO” should be understood as covering both genetically modified organisms as
defined under Article 2(2) of Directive 2001/18/EC, and genetically modified micro-organisms within the meaning of Article
2(b) of Directive 2009/41/EC.
4
Regulation (EU) No 536/2014 of the European Parliament and of the Council of 16 April 2014 on clinical trials on medicinal
products for human use and repealing Directive 2001/20/EC, (OJ L158, 27.5.2014, p.1). Until the Regulation applies,
Directive 2001/20/EC is applicable (Directive 2001/20/EC of the European Parliament and of the Council of 4 April 2001 on
the approximation of the laws, regulations and administrative provisions of the Member States relating to the
implementation of good clinical practice in the conduct of clinical trials on medicinal products for human use, OJ
L121,1.5.2001, p.34).
5
Directive 2001/18/EC of the European Parliament and of the Council of 12 March 2001 on the deliberate
release into the environment of genetically modified organisms and repealing Council Directive 90/220/EEC (OJ L 106,
17.4.2001, p. 1).
6
Directive 2009/41/EC of the European Parliament and of the Council of 6 May 2009 on the contained use of
genetically modified micro-organisms (OJ L 125, 21.5.2009, p. 75).

3
Austria:
Applicants should send separate submissions in case there are multiple sites concerned in Austria
(including clinical premises, laboratories in which activities with GMOs are carried out, locations of
storage of the investigational medicinal product and location of storage of samples from clinical trial
subjects that contain GMOs).
Further information is available at:
https://www.sozialministerium.at/site/Gesundheit/Gentechnik/Rechtsvorschriften_in_Oesterreich/
Belgium:
The common application form should be part of a biosafety dossier submitted by each of the clinical
sites where the investigational medicinal product will be administered. However, one person (e.g.
the sponsor) can be empowered by the concerned sites to submit all the necessary notifications,
provided that the person responsible for the activity is clearly indicated in the form.
More information on procedural requirements and forms for the three regions is available at:
https://www.biosafety.be/content/contained-use-gmos-andor-pathogenic-organisms-notification-
procedures.
Czech Republic:
Each clinical site as well as other institutions where the activities with GMOs will take place (e.g.
laboratories that are not premises of one of the clinical sites) should submit a separate notification
for deliberate release or for contained use, as appropriate. However, one person (e.g. the sponsor)
can be empowered by the concerned sites/institutions to submit all the necessary notifications.
France:
For investigational medicinal products that are assessed under the contained use framework,
applicants should send separate submissions in case there are multiple sites concerned in France.
Italy:
For investigational medicinal products that are assessed under the contained use framework, each
clinical site (including clinical premises, laboratories in which activities with GMOs are carried out,
locations of storage of the investigational medicinal product and location of storage of samples from
clinical trial subjects that contain GMOs) should submit a separate notification. However, one person
(e.g. the sponsor) can be empowered by the concerned sites/institutions to submit all the necessary
notifications.
It is stressed that, in case the submission is made by a third party on behalf of the site, the
responsibilities of the site holders and users concerned (as set out under Legislative Decree n.
206/2001) remain unchanged.
The Netherlands:
More information on national procedural requirements and forms is available at:
https://www.loketgentherapie.nl/en/aav
4
SECTION 1 – ADMINISTRATIVE INFORMATION
1.1. Identification of the applicant.
Organisation Name: Gyroscope Therapeutics Ltd.
Address Details: Rolling Stock Yard, 188 York Way, London N7 9AS, United Kingdom
Contact person: Kathryn Parsley
Telephone No:
+44 207 113 3691
Email Address:
k.parsley@gyroscopetx.com
1.2. Identification of the sponsor (to the extent that is different from the applicant).
Organisation Name:
Sponsor is as above (the applicant)
Address Details: Sponsor is as above (the applicant)
Contact person: Sponsor is as above (the applicant)
Telephone No: Sponsor is as above (the applicant)
Email Address: Sponsor is as above (the applicant)
1.3 Identification of the manufacturer of the clinical vector.
Organisation Name: Gyroscope Therapeutics Ltd. CMO: Catalent
Manufacturing
location:
Baltimore, USA
COMMON APPLICATION FORM FOR INVESTIGATIONAL MEDICINAL PRODUCTS FOR HUMAN
USE THAT CONTAIN OR CONSIST OF AAV VECTORs

5
SECTION 2 –INFORMATION RELATING TO THE INVESTIGATIONAL MEDICINAL PRODUCT
2.1. Description of the production system.
Clear maps of the vectors used for recAAV production (e.g. plasmids, baculoviruses) showing all the
constituent parts of the AAV clinical vector should be provided (i.e. in addition to the “transgene
vector”, all other vectors such as helper, packaging and pseudotyping vectors should be described).
The characteristics of all cell lines used and eventual modifications of the cell genome should be
explained. Describe the cell type(s) concerned as well as their origin (e.g. human kidney, epithelial
cells, insect cells).
The possibility of the genetic material in the cells/cell lines causing a certain interaction with the
clinical vector, such as by complementation or recombination should be discussed. In particular,
the tests applied to identify possible contamination of the cell line by wild-type AAV viruses and/or
any virus identified as helper virus for AAV should be explained.
GT005 is a recombinant, non-replicating, adeno-associated viral serotype 2 (rAAV2)
. The
expression cassette contains DNA encoding for human Complement Factor I (CFI), the therapeutic
transgene. The GMO is constructed using recombinant DNA technology from wild-type AAV2,
which is a non-pathogenic, single-stranded DNA genome containing, helper virus-dependent
member of the parvovirus family.
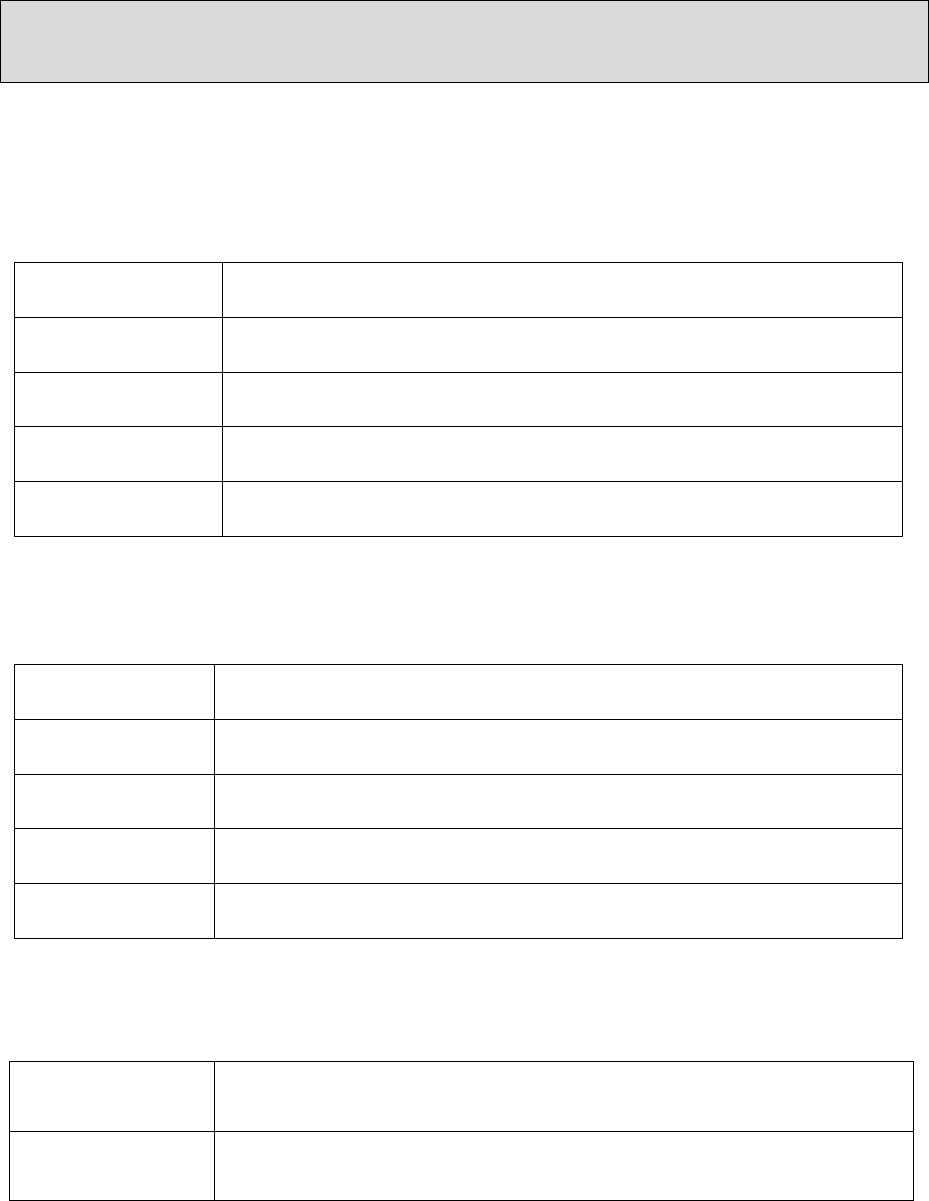
Description of production system
There are a number of strategies for the construction of an AAV gene therapy vector, one of which
is to separate the components required for AAV vector production on to small pieces of circular
DNA (plasmids) and to introduce these into a host cell. The plasmid which contains the DNA
sequence for the therapeutic transgene is typically referred to as a transfer plasmid and plasmids
which code for sequences required for vector construction within the host cell are referred to as
helper plasmids (Figure 1).
GT005 is manufactured for the Sponsor by a contract manufacturing organization (CRO) to GMP
via triple transient transfection of three plasmids (a helper, [pHELP Kan] and packaging plasmid
[pNLRep Cap2] and the transgene plasmid [pAAV2.CFI]) into a Human Embryonic Kidney (HEK) -
293T cell-line to produce high titre replication incompetent AAV that are free from adenovirus.

6
Figure 1. Schematic of plasmids used for AAV vector manufacture
Maps for the GT005 vector transfer plasmid pGT005 and the helper plasmids pNLRep_Cap2 and
pHELP Kan are considered confidential and are provided in a separate document (Annex 1 to the
Common Application Form – Confidential Information)
Possibility of recombination or complementation
Note that the required helper functions are provided as a plasmid, NOT a viable adenovirus.
GT005 is unable to replicate independently, even in the presence of a helper virus, since it lacks
the rep and cap genes required for rescue/packaging. Furthermore, unlike wild-type AAV2, rAAV
vectors devoid of the rep gene are incapable of site-specific integration into the AAVSl locus. In
the absence of REP protein, rAAV vectors such as GT005 persist extra chromosomally in non-
dividing cells as episomes. There is an absence of homologous sequences on the vector transfer
and helper plasmids to reduce the likelihood of generating replication competent AAV2 during
manufacture.
All plasmids used for the production of GT005 have been fully sequenced by double stranded
primer walker sequencing or next generation sequencing (NGS) to confirm sequence identity.
Each batch of GT005 is also sequenced as part of release testing for each plasmid batch.
Therefore, the identity of GT005 and absence of unintended sequence modifications is assured.
Infection with wild-type AAV is asymptomatic and AAV is not known to cause any noticeable
pathology [Flotte and Berns, 2005]. Therefore, given the non-pathogenic nature of the virus in
humans, no specific treatments have been developed.
The genetic modifications made to generate GT005 do not change the non-pathogenic nature of
AAV2 and equally, the modifications are not anticipated to have any effect on the host range,
stability or survival of the GMO outside of the host when compared to that of the wild-type virus.

7
A theoretical risk of AAV infection is the risk of insertional mutagenesis caused by site-specific
(AAVS1) integration of the AAV genome into the host-cell genome of infected human cells.
Although no integration studies have been performed using GT005 specifically, numerous
integration studies have been performed evaluating the integration frequency, and integration
sites of AAV2 vectors. AAV integration patterns have been evaluated by linker-mediated PCR (LM-
PCR) and linear amplification PCR (LAM-PCR) in transduced cells in mouse liver [Kaeppel et al.,
2013; Li et al., 2011], NHP muscle and liver [Nowrouzi et al., 2012], and human muscle [Kaeppel
et al., 2013]. These studies confirmed the low frequency of integration, and there was no evidence
of AAV vectors causing insertional activation of oncogenes and subsequent tumor formation. Li
et al. observed integration patterns demonstrating preferential integration into actively
transcribed genes, CpG islands and GC-rich, although this was not observed by Nowrouzi et al. or
Kaeppel et al. Further, multiplex-LAM PCR was used to identify and quantify integration sites (IS)
in NHP tissue and human liver biopsies following intravenous administration of an AAV vector
[Gil-Farina et al., 2016]. Integration frequencies ranged from 1x10
-4
to 7.44x10
-5
IS/cell in NHP
tissue, and 1.17x10
-3
to 2x10
-4
IS/cell in human liver samples. Additionally, no integration clusters
or events were found in genes previously reported to link AAV integration with hepatocellular
carcinoma development, demonstrating the lack of genotoxicity of systemically administered AAV
vectors.
It is important to note that the integration mechanism of AAV differs from that of other viruses,
such as retroviruses. Retroviral vectors contain the integrase protein needed to cause double
stranded breaks for integration [Lesbats et al., 2016], whereas AAV vectors do not contain such
proteins and must rely on the cellular machinery [Miller et al., 2004].
AAV vectors do not encode proteins that catalyse integration and have to rely on cellular factors
to integrate into pre-existing breaks [Miller et al., 2004]. Therefore, the risk of AAV vector-induced
insertional mutagenesis or carcinogenesis, particularly in post-mitotic cells such as retinal cells, is
considered low.
Clonal integration of wild-type AAV2 into known cancer-causing genes have been found in 11 of
193 hepatocellular carcinoma, suggesting a possible role of wild-type AAV2 in liver carcinogenicity
by insertional mutagenesis in humans [Nault et al., 2015]. Importantly, most of the integration
events included the 3’ portion of the wild-type AAV capsid gene which is not present in AAV2
vectors. Additionally, unlike the wild-type AAV2 integration described by Nault et al., GT005 is
administered at a relatively low dose to post-mitotic tissue on a single occasion. There is no
evidence from non-clinical studies that exposure of cells to GT005 causes abnormality in cell
growth, metabolism or surface growth properties, and no systemic toxicities were observed in
non-clinical studies. Furthermore, Spark Therapeutics are collecting long-term safety data from
patients who received subretinal injections of the AAV2-based product, voretigene neparvovec
[Luxturna, FDA, 2017], at a dose of 1.5x10
11
vg/eye and have not reported any incidences of
tumorigenesis.
In the case of transfer of vector to an unintended human recipient, these risks are expected to
be considerably reduced, since the vector is not able to replicate and the dose which may
conceivably be transferred via the aforementioned routes will be orders of magnitude lower
than that received by patients. The components of the AAV2 vector GT005 are based on the
publicly disclosed construct developed by Nightstar Therapeutics (rAAV2.REP1) for the
treatment of Choroideremia [Dimopoulos et al., 2018]. GT005 differs from the Nightstar

8
Therapeutics vector only by the transgene being expressed, i.e., CFI rather than Rab escort
protein 1 (REP1) cDNA sequence.
Characterisation of cell lines used for production
The human cell line HEK293T is used for the production of GT005 vector. HEK293 cells were
originally generated [Graham et al., 1977]
through the transformation of normal human
embryonic kidney cells with sheared adenovirus type 5 DNA. The HEK293T cell line was derived
from the parent HEK293 cell line [Rio
et al., 1985] and contains the temperature sensitive allele
of the SV40 large T-a
ntigen (SV40Tts) which increases the expression levels obtained with
transient transfection [Geisse and Fux, 2009]. A risk assessment of the SV40Tts gene present in
HEK293T cell line indicates that there is an extremely low risk to human health.
The HEK293T Master Cell Bank (MCB) was manufactured in accordance with GMP and stored at
<120°C. The MCB was extensively characterised consistent with EU guidelines and pertinent Ph.
Eur. Chapters for the absence of in vitro and in vivo adventitious agents and to confirm the identity
and viability of the cell stock.
2.2. Demonstration of absence of formation of replication-competent virus.
The risk of generation of a replication competent AAV through recombination of the constituent
parts of the viral vector system should be minimised. Test methods for detection of replication-
competent virus should be described including information on the specificity and sensitivity thereof.
Data from RCV testing at different manufacturing steps should be provided (e.g. virus seed bank,
final product). Release criteria with regard to RCV testing should be specified.
Risk of rcAAV generation and its mitigation
Due to minimal construction of GT005 genome and separate plasmid system used for GT005
production, formation of replication-competent virus is minimised.
With reference to the description of the production system provided in Question 2.1, the
construction of the GT005 genome (ITRs and transgene only) and the manufacturing process
(using a three-plasmid system without sequence homology) have been designed such that the
generation of replication competent AAV2 through homologous recombination is remote. As
such, GT005 is unable to replicate independently, even in the presence of a helper virus, because
it lacks the rep and cap genes required for rescue/packaging.
Exposure to rcAAV may theoretically be mediated by the investigational product by either
generation of rcAAV
by recombination of (sequences from) production plasmids during
manufacture, or homologous recombination of an existing wild-type AAV with GT005 in a patient's
cells (co-infected with a helper virus). In terms of rcAAV, the potential routes of exposure will be
the same as for GT005, however the likelihood of transmission of rcAAV is considered even lower
than that of GT005, given that GT005 is tested for the absence of rcAAV as part of QC testing prior
to the release of the product for use. The likelihood of a homologous recombination event in vivo
is also very low, requiring a triple infection of the same cell, followed by a recombination event.
Furthermore, the regions of homology between GT005 and wild-type AAV are limited to the ITRs
since the rep and cap genes are deleted from the recombinant vector.

9
The genetic material from the rep and cap genes together with the transgene would be too large
in size to be packed in an AAV capsid. Thus, it is highly unlikely that the recombination would result
in a replication-competent vector containing the transgene. Any recombination would result in
the expression of the transgene by infected cells.
The genetic traits of the modified organism are expected be stable considering the known genetic
stability of the parent wild-type AAV and also because the therapeutic activity of GT005 is not
dependent on replication of the AAV vector.
Homologous recombination between GT005 and wild-type AAV could occur if both were present
in the same cell that was also infected with a helper virus. Such recombination could only result
in the exchange of the transgene expression cassette with the rep and cap genes of the wild-type
virus. However, it is not possible for the AAV genome to contain both rep/cap genes and the
transgene, as this is beyond the packaging limit of the virion. Moreover, the regions of homology
between GT005 and a potential co-infecting wild-type AAV would be limited to the ITRs, since the
rep and cap genes have been removed from GT005; this is therefore likely to further decrease the
possibility of recombination.
The only mechanism by which the transgene would be mobilised is through a triple infection of
the same cell by GT005 (containing the transgene), wild-type AAV (providing the Rep and Cap
functions) and a helper virus. It this occurred, it would result in the production of further wild-
type AAV and further GT005 vector particles, which could still lack the rep and cap genes and
would thus not be self-sustaining.
Detailed description of rcAAV detection method, its sensitivity, specificity and associated release
criteria. are considered confidential and are provided in a separate document (Annex 1 to the
Common Application Form – Confidential Information)
2.3. Provide a diagram (‘map’) of the clinical vector.
A schematic of the GT005 vector genome is provided in the schematic below. For a description of
each element within the genome, see Question 2.5.
Schematic of the GT005 vector genome
Abbreviations: ITR - inverted terminal repeat, CBA - chicken β-actin promoter, CFI - Complement Factor I cDNA, WPRE
- Woodchuck post-transcriptional regulatory element, bGHpA - bovine growth hormone polyadenylation signal.
2.4. Molecular characterisation of the clinical vector
Provide the annotated sequence of the genome (i.e. indicate the location of the sequences
encoding the transgene expression cassette(s) and its regulatory elements).

10
Describe in what way the clinical vector deviates from the parental virus at the level of molecular
characterisation.
Available data supporting genetic stability of the clinical vector should be provided. Deviations
should be discussed, in particular the biological significance thereof.
Molecular characterisation of the parental virus
Wild-type AAV have a linear positive or negative single-stranded DNA genome approximately 4.7
kilobases (kb) long. The genome consists of two coding elements: the replicase (rep) gene which
encodes Rep78, Rep68, Rep52 and Rep40, proteins required for AAV replication and packaging,
and the capsid (cap) gene encoding the capsid proteins VP1, VP2, and VP3 (Figure 1). These
elements are flanked by two identical inverted terminal repeats (ITRs) which function to package
the single-stranded DNA into virions and also in protecting and maintaining the unpackaged DNA
in an episomal state in transduced cells.
The parental virus of GT005 is adeno-associated virus serotype 2 (AAV2). AAV2, one of several
species in the Dependovirus genus of the Parvoviridae family, requires helper functions supplied
by co-infecting helper viruses to enable productive infection. AAVs are small (approximately 25 nm
in diameter), non-enveloped, non-
pathogenic viruses which infect cells through a receptor
mediated process after which the viral DNA is transported to the nucleus. Wild-type AAV is
naturally replication-deficient as it relies on co-i
nfection with other types of virus, mainly
adenoviruses.
Figure 1. Adeno-associated virus (AAV) genome map (schematic)
(Figure taken from Vector Biolabs https://www.vectorbiolabs.com/intro-to-aav/
)
The characteristics present in the virus genome that identify it as an AAV2 derivative are the ITR
sequences present on the vector transfer plasmid, and the rep and cap genes present on the helper

11
plasmid. The primary reference for the ITR, and rep and cap gene sequences is GenBank J01901.1
(AAV2 complete genome and the sequence identity was confirmed as 100%).
The presence of AAV may be detected in five ways:
Molecular Technique: Polymerase Chain Reaction (PCR). PCR can be used to detect vector genome
sequences associated with AAV in a qualitative or quantitative manner, using primers specific for
the rep or cap genes. Detection of a specific serotype, or any AAV-like sequence, as well as
distinction between wild type AAV and recombinant AAV is possible, depending on the choice of
primers. Note that the presence of vector genomes does not necessarily imply infectious virus
particles.
Molecular Technique: Next Generation Sequencing (NGS). NGS can be used to detect vector
genome sequences associated with AAV in a qualitative or quantitative manner, using a sequencing
library from the sample. Detection of a specific serotype, or any AAV-like sequence, as well as
distinction between wild type AAV and recombinant AAV is possible. Note that the presence of
vector genomes does not necessarily imply infectious virus particles.
Immunological technique: As AAV capsid proteins can be detected electrophoreti
cally by a
semiquantitative method using sodium dodecyl sulphate -polyacrylamide gel electrophoresis (SDS-
PAGE) and identified using Western Blot with antibodies’ specific to the tree viral coat proteins of
AAV. The identification is based on visual assessment by comparing the banding patterns from the
test sample e.g., recombinant AAV to that of a qualified reference standard (wild-type AAV).
Immunological technique: Enzyme-
Linked Immunosorbent Assay (ELISA) methods which are
quantitative are used to detect AAV vector particles relying on the generation of specific antibodies
to the vector capsid proteins, and can therefore be specific to an individual serotype, or cross react
with several AAV serotypes. Detection of vector capsid particles does not necessa
ry imply
infectious virus particles.
Co-culture: Samples containing suspected infectious AAV particles may be cultured in vitro on a
permissive cell line, in the presence of a helper virus.
The sensitivity/specificity of the methods for detection of wild type AAV described above is not
significantly detailed in the scientific literature, most likely due to a lack of clinical utility of
diagnostic methods given the apparent lack of pathogenicity of the virus. In more recent years, the
literature details detection methods of recombinant AAV based vectors that are being developed
as gene therapy medicinal products.
PCR and ELISA -based detection methods can be designed to be highly specific for a specific AAV
serotype, through the selection of specific primers/probes or antibodies. Conversely, the methods
can be designed to target conserved regions to detect a broad range of serotypes.
Genetic stability of the clinical vector
The GT005 vector genome is a “gutted” wild-type genome, as it does not contain the rep and cap
genes, only the transgene and the ITR sequences, as described in Questions 2.3 and 2.5. Thus,
GT005 is replication-defective, even in the presence of a helper virus.
Wild-type AAV is a non-enveloped virus, with a stable capsid. The genetic modifications made to
generate GT005 are not anticipated to have any effect on the host range, stability, sensitivity to

12
inactivating agents or survival of the GMO outside of the host when compared to that of the wild-
type virus. There have been extensive studies on AAV vectors showing that exposure to heat, UV
radiation, or extreme pH can inactivate recombinant vector particles. For example, AAV particles
are resistant to pH 3-9 and can resist heating at 56
o
C for 1 hour [Berns and Bohenzky, 1987].
Infection with wild-type AAV is asymptomatic and AAV is not known to cause any noticeable
pathology [Berns and Parrish, 2007; Flotte and Berns, 2005; Zinn and Vandenberghe, 2014].
Although human infections are common, AAV is not known to be a pathogenic virus in humans
[reviewed in Srivistava 2016]. AAV has never been implicated as an etiological agent for any
disease [Blacklow et al., 1968a, 1968b, 1971]. Furthermore, AAVs are dependent on co-infection
with other viruses, mainly adenoviruses, in order to replicate [Berns and Parrish, 2007]. Wild-type
AAV can infect host cells and release its genome to the host cell nucleus. However, in the absence
of a helper virus, it remains dormant.
Wild-type AAV-2 is non-pathogenic, and it is designated a Risk Group 1 biological agent, defined
in the EU as 'one that is unlikely to cause human disease'. The parental AAV is of low hazard and
can therefore be handled at Containment Level 1. It is not classified in Risk Groups 2, 3 or 4
according to Directive 2000/54/EC on the protection of workers from risks related to exposure to
biological agents at work (Annex III of the Directive).
GT005 (rAAV2 vector) is considered low risk since it has been engineered to be replication
incompetent by modifications to the genome. The vector particles are manufactured using
sequences for the genome, packaging and helper components separated between three plasmids.
Furthermore, each vector (GT005) batch is tested for replication competent virus (rcAAV) as part
of routine product QC release testing.
In general DNA viruses have greater genetic stability than RNA viruses. However, GT005 is unable
to replicate, even in the presence of a helper virus since the genes essential for replication are
deleted. The genetic modifications made to generate GT005 do not alter the stability of the viral
vector compared to wild-type AAV2. The stability in terms of genetic traits is therefore expected
to be equivalent to wild-type AAV. DNA of wild-type AAV and of AAV-based vectors persists in
transduced cells as circular (extrachromosomal) episomal concatemers in human tissues [Chen et
al., 2005, Schnepp et al., 2005, Schnepp et al., 2009]. However, due to the lack of viral rep and cap
genes, GT005 is expected to remain in the cells as episomes and will not replicate and produce
viral particles.
2.5. Description of the insert
The expression cassette e.g. transgene, including regulatory and coding sequences, should be
described. In particular, it should be explained if the expressed product is toxic or otherwise
harmful to humans (other than the clinical trial subject) or other hosts. Additionally, if the
applicant considers that the transgene could confer any advantage for replication/survival of the
clinical vector (vis-à-vis the parental virus), this should be explained.
A description of the expression cassette showing the transgenes and regulatory regions is provided
in Question 2.3. A description of each element is provided below.

13
INVERTED TERMINAL REPEATS (ITRS)
The 5’ and 3’ terminal regions of the vector genome contain inverted terminal repeats known as
ITRs. These sequences which are identical in sequence to the viral genome of wild-type AAV-2 are
self-complementary and form hairpin structures [Samulski et al., 1987]. The ITRs are required for
packaging of the viral genome into the particles and after transduction of the target cells, for
stabilisation of the viral genome. The ITRs initiate complementation of the (unstable) single
stranded genome DNA into (stable) double stranded DNA by host cell polymerases. Alternatively,
because the ITRs are palindromic, multiple viral genomes can assemble ITR to ITR to form larger
double stranded DNA structures known as concatemers. These concatemers remain
transcriptionally active and stable episomal structures [Schnepp et al., 2005]. The ITRs do not
contain any open reading frames for protein expression and. directly flank the expression cassette.
CYTOMEGALOVIRUS (CMV) ENHANCER
CMV Enhancer is fused to CBA to provide optimal expression of the CFI transgene.
CHICKEN β-ACTIN PROMOTER (CBA)
The strong ubiquitous CBA promoter was used for the vector to provide high expression of the CFI
transgene. Effective transduction was observed in retinal gene therapy clinical trials [Cideciyan et
al., 2008; Hauswirth et al., 2008].
TRANSGENE: COMPLEMENT FACTOR I (CFI)
The transgene is CFI, a serine protease that is essential for regulating the complement alternative
pathway. It is responsible for the cleavage and inactivation of components in the complement
system (CS) and preventing the assembly of the convertase enzymes. Mutations in the CFI gene
have been associated with a predisposition to develop diseases associated with complement
system dysregulation, including Age-related Macular Degeneration (AMD).
The sequence of the transgene is identical to the open reading frame in NCBI Reference Sequence:
NG_007569.1.
WOODCHUCK HEPATITIS VIRUS POST-TRANSCRIPTIONAL CONTROL ELEMENT (WPRE)
The woodchuck hepatitis virus post-transcriptional control element (WPRE) is also included and is
intended to enhance transgene expression [Patricio et al., 2017]. The WPRE sequence is modified
to abrogate promoter activity and start codon of Woodchuck hepatitis virus X protein which has
been associated with tumorigenesis in hepatocellular carcinomas [Kingsman et al., 2005].
BOVINE GROWTH HORMONE POLYADENYLATION SIGNAL (bGHpA)

14
The bovine growth hormone polyadenylation signal (bGHpA) is used as a polyadenylation signal
and transcription termination sequence.
ORIGIN OF SEQUENCES INCORPORATED INTO GT005 VECTOR PARTICLES
The DNA sequences are generated in
vitro using molecular biological techniques. These are
transcribed from the transfer plasmid.
Description of genetic trait(s) or phenotypic characteristics and in particular any new traits and
characteristics which may be expressed or no longer expressed
The host range, tissue specificity, and tropism of AAV is determined by the capsid. The capsid of
GT005 is composed of the same proteins as wild-type AAV2, therefore, the host range and tropism
of GT005 vector and wild-type AAV2 are the same.
Infection with wild-type AAV is asymptomatic; AAV is not known to cause any noticeable pathology.
Given that the structure and thus the potential to infect will not have changed, it is expected that
the safety profile of the parental wild-type AAV and GT005, are similar. In addition, GT005 lacks
the rep and cap genes present in wild-type AAV2 therefore the vector is replication-defective. Even
in the presence of helper virus, the vector genome of GT005 will not be replicated, nor will capsids
be formed. The two processes associated with wild-type AAV infection (i.e., replication and capsid
formation) will not take place after infection with GT005. The safety profile of GT005 is therefore
theoretically more favourable compared with that of wild-type AAV.
As with voretigene neparvovec (EPAR, EMEA/H/C/004451/0000), in respect of biodistribution,
following subretinal injection no systemic exposure to AAV2 is expected and the transgene is not
expected to be expressed except in tissue that is both exposed to virus and has the necessary
components to make CFI protein.
PHARMACOLOGICAL ACTIVITY OF GT005
Following subretinal administration of GT005 and delivery of GMO-derived DNA to the nucleus, the
therapeutic transgene is transcribed and translated, and human CFI protein is produced by the
retinal pigmented epithelium cells. The retina is a natural source of CFI protein, i.e., the transgene
is expressed in a natural environment. Thus, local adverse responses to GMO-mediated CFI
expression are not expected.
PERSISTENCE AND INTEGRATION OF GT005
In the absence of REP protein rAAV vectors persist extra chromosomally in non-dividing cells such
as retinal pigment epithelium (RPE) cells as episomes. The possibility of integration events is
extremely rare (- 0.1%), however random insertion site distribution may exist [Salmon et al., 2014]
.
Data on biodistribution have been obtained for GT005 as part of the GLP NHP toxicology study. A
validated, GLP-compliant, qPCR assay was used for measuring the number of copies of GT005 in
aqueous humor, heart, kidney, liver, lung, optic chiasm, optic nerve, optic tract, ovary, retina, RPE
and choroid at and outside the dose site, spleen, testes and vitreous humor samples, 183 days after
dosing.
The overall biodistribution pattern between both GT005 dose groups was similar, with the dose
site yielding the highest concentrations with an average concentration of 1.7x10
7
and 3.6x10
7
copies in the low dose and high dose groups, respectively. The low dose samples from outside the
15
dose site and the vitreous humor samples from the high dose group had the next highest
concentrations at 2.0x10
5
and 3.9x10
4
copies, respectively. Aside from the dose site, the levels of
GT005 across the biodistribution samples were comparable between the low and high dose groups.
Spleen samples demonstrated sporadic and relatively low concentrations of GT005, while the
heart, kidney, liver, lung, ovary, and testes samples all tested below the assay limit of detection
(BLOD), indicating a lack of sustained and systemic vector spreading or biodistribution 183 days
after a single subretinal injection of GT005.
Numerous integration studies have however been performed evaluating the integration frequency,
as well as the integration sites, of rAAV vectors. Integration has been shown to occur preferentially
into RefSeq genes, CpG islands, near transcription start regions, into rRNA gene repeats, and in
some studies, DNA palindromes [Inagaki et al., 2007; Miller et al., 2004; Nakai et al., 1999; Nakai
et al., 2003; Nakai et al., 2005]. It was also suggested that AAV vectors integrate at pre-existing
chromosome breaks, rather than causing breaks themselves [Miller et al., 2004]. Based on current
knowledge, GT005 is concluded to present a similar risk with respect to genomic integration when
compared to wild-type AAV.
HOST IMMUNE RESPONSES TO GT005
The host immune response to GT005 is not expected to be different from wild-type AAV2, as
reviewed in Daya and Berns (2008). Interim clinical immunogenicity data on GT005, as of
December 2020, show that antibodies to CFI have not been detected in any subject and at any time
point. One subject had a transiently positive anti-AAV2 T cell response, which was absent at Week
24 post-treatment. No positive T cell response to AAV2 was detected for all other patients. Almost
no innate immune response is seen in AAV infection and the host defence mechanism at the
adaptive level is primarily made up of a humoral response [Xiao et al., 1996]. Pre-existing
antibodies, due to prior AAV infections, account for the observed humoral response in patients
receiving rAAV vectors (reviewed in Ertl and High, 2017). The cell-mediated response functions by
eliminating transduced cells through cytotoxic T cells. Cell-mediated responses to AAV vectors
have been documented, but may be dependent on several factors, including the vector dose, route
of administration, and prior exposure to the AAV serotype [Ertl and High, 2017]. Subjects treated
with GT005 will therefore be given prophylactic corticosteroids around the time of the subretinal
injection of the GMO to treat potential immune reactions.
Doses used in ophthalmo
logy are considerably smaller than other applications such as in
haematology, where doses in the range of E13 vg/kg are used and, when compared to systemic
delivery of AAVs targeting organs such as the liver, the eye represents a site of immune privilege.
Nevertheless, intraocular inflammation following subretinal delivery of AAV gene therapy in
humans has been recorded, however it is usually not clinically significant and is readily controllable.
In the Phase II study, the highest proposed dose of GT005 is 2E11 vg and as mentioned above
subjects treated with GT005 will be given prophylactic corticosteroids around the time of the
subretinal injection of the GMO to treat potential immune reactions.
Immunological reactions are nevertheless rare following AAV injection into the subretinal space.
AAVs elicit a minimal immune response and allow for stable and long-term transgene expression
in different retinal cells, including photoreceptors, retinal pigment epithelium (RPE) cells, ganglion
and Muller cells [Vandenberghe and Auricchio, 2012]. Exposed individuals could seroconvert to an
AAV2-positive titre. There has been no indication from any of the previous AAV human trials that

16
this humoral response (neutralising antibodies) against the capsid proteins has any apparent
clinical sequelae other than the potential to reduce effectiveness of a future AAV gene therapy
administration.
SUMMARY
Altogether as infection with wild-type AAV already does not result in any noticeable pathology and
CFI is expressed in its natural environment, the safety profiles of GT005 and the parental strains
will be similar, in that neither will mediate any noticeable pathological effects. Since infection with
wild-type AAV is asymptomatic and AAV is not known to cause any noticeable pathology, treatment
methods against the GMO are not considered relevant.
Considerations for human health and animal health, as well as plant health environmental
exposure to GT005:
The potential for unintended spread within the environment is considered low. Transmission of
GT005 to an unintended human recipient is likely to be isolated since the product will be
administered to and handled by a limited number of individuals in a hospital environment. Any
inadvertent exposure will be self-limiting, GT005 is replication defective, even in the presence of a
helper virus, as it lacks the rep and cap genes required for rescue/packaging. The likelihood of
GT005 to become persistent or invasive is therefore negligible.
Furthermore, the transgene (CFI) is not expected to confer any advantage to GT005 in terms of
survival in the environment. None of the genetic modifications made to wild-type AAV2 during
construction of GT005 would be expected to enable the transfer or maintenance of genetic
material into the environment (outside its obligate host species) or have an effect on sensitivity to
inactivating agents or survivability in the environment. The potential for environmental
interactions with non-target organisms is therefore considered negligible.
The likelihood of gene transfer to species other than humans and (some) primates is low, given the
host range of AAV. The natural host of wild-type AAV2 is humans. AAV does not infect plants or
other microbes. As far as (unintentional) gene transfer to humans and primates is concerned, the
likelihood is low given that GT005 is modified from wild-type AAV2 and is unable to replicate
independently, even in the presence of a helper virus, as it lacks the rep and cap genes required
for rescue/packaging. These genetic modifications do not affect its natural host range and tissue
tropism.
No immediate and/or delayed environmental impact is expected. The potential for environmental
impact of the interactions between GT005 and humans is negligible. Wild-type AAV2 is not known
to be involved in environmental processes. It does not respire and does not contribute to primary
production or decomposition processes. It does not display any metabolic activity in its virion form.
GT005 will be administered subretinally to eligible patients by trained medical professionals in a
hospital environment. The procedure will involve standard 3 port pars plana vitrectomy with a core
vitrectomy followed by subretinal delivery. The potential for direct exposure will be limited to
those healthcare professionals involved and trained in dose preparation and administration.
Procedures are in place to minimise this risk. The likelihood of secondary exposure to close
contacts of patients who receive the treatment (including family members, caregivers) is also
considered very low.

17
Due to the low numbers of vector DNA copies potentially expected to be released into the
environment through shedding, horizontal gene transfer is highly unlikely. Even if horizontal gene
transfer occurred, the sequences would not confer a selective advantage to other organisms such
as bacteria since GT005 does not contain any prokaryotic promoters, any antibiotic or other types
of resistance genes or any genes, which would enhance or constrain their growth. Therefore, it is
unlikely that GT005 would interfere with the control of pathogenic microorganisms or that it would
have an effect on the natural dynamics of microbial populations or the biogeochemical cycles at
any given site in the environment.
2.6. Biodistribution and shedding
Detailed data on clinical vector shedding (including information on the administered dose, the
route of administration, and –where available- immune status of the treated subjects) from
previous clinical trials with the clinical vector should be provided. Where available and if relevant
for the environmental risk assessment, biodistribution data should be provided.
If there is no prior clinical experience with the same clinical vector, the potential for shedding
should be discussed based on non-clinical data and/or clinical experience from related clinical
vectors. If the applicant relies on data from related clinical vectors, the relevance of the data to
the product that is the object of this application should be explained considering, in particular,
the dose and route of administration.
When shedding occurs, the estimated duration should be specified.
The methods used for detection of viral shedding, including information on the specificity and
sensitivity thereof, should be provided.
Clinical vector shedding potential
The survival and route of transmission of the AAV construct is not expected to be different from
that of wild-type AAV. The route of exposure will therefore most likely be through direct contact
with the gene therapy product, as opposed to from potential secondary exposure resulting from
shedding of the vector from treated patients.
GT005 cannot replicate in the human body, and shedding is anticipated to be low level and
transient, based on a non-
clinical assessment with GT005 and clinical experience with other
subretinally delivered rAAV2 products. Subjects enrolled in clinical trials with GT005 are asked to
use two forms of contraception, one of which being a barrier method for 90 days post-dosing, if
relevant. Wild-type AAV dissemination is mainly through the airway, although sexual transmission
has been hypothesised. GT005 vector is replication-deficient even in the presence of a helper virus
infection but rcAAV can theoretically be formed during production of the GMO, although risk of
rcAAV formation is predicted to be negligible. In the event that wild-type/replication-competent
AAV is formed, this is not expected to result in pathology/disease symptoms as infection with AAV
is asymptomatic. Therefore, the GMO or sequence derived from the GMO, are not likely to
replicate within the recipient following administration and therefore the absolute amount of GMO
that could theoretically be shed would not exceed the dose administered. Spread of the GMO is

18
not facilitated through helper functions, presence of rcAAV, or recombination events between the
GMO and wild-type AAV.
Viral vector shedding is expected to be minimal with GT005 and in line with the shedding profile
observed with other subretinally administered AAV-based products [EPAR public assessment for
Luxturna, 2020]. Shedding analyses from a non-clinical assessment of GT005 and in previous clinical
trials using similar AAV dosages and identical route of administration (sub-retinal injection) e.g.,
Nightstar Therapeutics (rAAV2.REP1) report very limited detection of vector DNA in body fluids.
Additionally, GT005 will be injected into the subretinal space and the viral vector is replication
incompetent. Due to the low numbers of vector DNA copies potentially released into the
environment through shedding, horizontal gene transfer is highly unlikely. The likelihood of
secondary exposure through vector shedding is also low, due to the inability of the vector to
replicate (even in the presence of helper virus) and the low and transient levels of vector shedding
anticipated.
Vector shedding data was collected for the construct as part of a toxicity study using non-human
primates (NHP) and intended to mimic the route of administration to be used in the clinical study.
A qPCR assay was used to measure the number of copies of GT005 in blood, tears and saliva
samples. The results from the blood and saliva samples had the highest concentration at the initial
timepoint and decreased over time with each successive interval. The vector shedding pattern in
tear samples was similar to the blood and saliva samples with a decrease in concentration over
time. All blood samples had the lowest concentration with only a single sample in each treated
dose group at Day 3 within the quantifiable range of the assay and at Weeks 13 and 26 were below
the limit of detection (BLOD). For saliva samples, on Day 3, three animals from the high dose group
had quantifiable vector concentrations of 3,485, 10,346, and 61,776 copies and by Week 4 all saliva
samples from all animals tested BLOD. All tear samples tested BLOD by Week 13 with the exception
of a single sample which was below the level of quantification but detectable.
Clinical vector shedding from previous clinical trials of GT005
The FOCUS (GT005-01) study is a first in human, Phase I/II, open-label study evaluating the safety,
dose response and efficacy of GT005 administered as a single subretinal injection in the study eye
in subjects with bilateral geographic atrophy (GA) due to age-related macular degeneration (AMD).
The assessment of vector shedding is being conducted as part of this Phase I/II clinical study and the
available interim shedding data from Cohorts 3 and 4 was available as of October 2021, following
the initial application to the EPA.
Blood, urine, saliva and tears (from both the treatment eye and the contralateral eye) were collected
at screening, 12-24 hours post-GT005 administration, and at week 1 and week 4. Based on interim
data (as of Oct 2021) on vector shedding from patients treated in Cohorts 3 and 4 (medium or high
dose) in the GT005 Phase I/II FOCUS clinical study, clinical vector is expected to be cleared (no
further shedding) from patients within week 1 of treatment. These data are in line with the shedding
profile observed with other subretinally administered AAV-based products (EPAR public assessment
for Luxturna, 2020).

19
Overall, the likelihood of horizontal gene transfer through vector shedding is low, due to the inability
of the vector to replicate (even in the presence of helper virus) and the low and transient levels of
vector shedding observed.
Treatment with the construct is a local therapy with very low risk of systemic distribution of the
vector, as evidenced by the non-clinical assessment and by other studies following subretinal AA
V2 administration at a similar dose [Maguire et al., 2009; Maclaren et al., 2014; Bainbridge et al.,
2015]. Based on the above and the findings by others [EPAR public assessment for Luxturna, 2020],
it is concluded that no specific risk management measures are deemed necessary for the two Phase
II studies (EXPLORE and HORIZON).
Specificity of the qPCR detection is
considered confidential and are provided in a separate
document (Annex 1 to the Common Application Form – Confidential Information)
SECTION 3 –INFORMATION RELATING TO THE CLINICAL TRIAL
3.1. General information about the clinical trial.
EudraCT-number
(where available):
2019-003421-22 (EXPLORE) and 2020-002431-30 (HORIZON)
Deliberate release
reference number
(where available and
applicable):
B/IE/21/01
Title of the clinical
trial:
EXPLORE: A Phase 2, Outcomes Assessor-Masked, Multicentre,
Randomised Study to Evaluate the Safety and Efficacy of Two
Doses of GT005 Administered as a Single Subretinal Injection in
Subjects with Geographic Atrophy Secondary to Age-Related
Macular Degeneration
HORIZON: A Phase II, Open-Label, Outcomes-Assessor Masked,
Multicentre, Randomised, Controlled Study to Evaluate the Safety
and Efficacy of Two Doses of GT005 Administered as a Single
Subretinal Injection in Subjects with Geographic Atrophy
Secondary to Dry Age-Related Macular Degeneration
Name of principal
investigator:
Dr. Eugene Ng

20
Objective of the
study:
The overall objectives of the studies are to evaluate the safety
and efficacy (anatomical and functional visual outcomes) of
three doses of GT005 in genetically defined subjects with
Geographic Atrophy due to Age-Related Macular
Degeneration
Intended start and
end date:
Start: June 2022
End: July 2026
Number of trial
subjects that will take
part in the study:
Approximately 30 patients across both the EXPLORE and HORIZON
studies.
Indicate if an
application related to
the same
investigational
medicinal product has
been submitted -or is
planned to be
submitted- to other
EEA Member States.
In the affirmative,
identify the countries
concerned:
Clinical trial applications have been submitted to the following EEA
Member States:
• France
• Germany
• Netherlands
• Spain
• Poland
3.2. Intended location(s) of the study.
The applicant should provide information about the sites located in the country of submission
of the application.
In some jurisdictions, the following additional information should be provided:
• the location(s) of laboratories (in the country of submission) in which activities with the
GMO are carried out under the framework of the clinical trial application should be stated
.
7
• information about the location where the investigational medicinal product is stored (to
the extent that the location is in the country of submission but outside the clinical site).
8
• information about the location where patient’s samples that contain GMO’s are stored
(to the extent that the location is in the country of submission but outside the clinical
site).
9
Organisation
Name:
UPMC Whitfield Hospital Institute of Eye Surgery
Address Details:
2 Butlerstown, Waterford, X91 DH9W, IRELAND

21
Contact person:
Helen Carty
Telephone No:
+353-51-552050
Email Address:
Planned
activities:
Storage, preparation, and administration of the ATIMP. Patient follow
up.
Containment
level:
Containment Level 1
Name and
contact details of
the responsible
person
10
:
See contact person as above
7
Information about the location of laboratories is required for applications submitted to Austria, Belgium,
Croatia, Czech Republic, Denmark, Finland, France, Germany, Hungary, Ireland, Portugal and Spain. In case
of submissions to these jurisdictions, fill in the relevant table for laboratories that conduct specialised
analysis referred in the protocol of the clinical trial only; laboratories that perform standard laboratory
diagnostics analysis need not be listed.
8
This information should be provided for applications submitted to Croatia, Germany, Ireland and Spain.
This
information should be provided for applications submitted to Belgium, Czech Republic and Finland,
unless there is a contained use notification covering the storage of the product.
9
This information should be provided for applications submitted to Germany and Ireland.
10
The responsible person is either the person responsible for supervision and safety as provided for under
Annex V of Directive 2009/41/EC, or the responsible scientist as provided for under Annex IIIA of Directive
2001/18/EC.
(Applicant should complete as many tables as necessary)
3.3. Storage of the clinical vector at the clinical site.
The applicant should provide information about the storage location, conditions of storage
(including restrictions of access), and the maximal storage duration.
11
The IMP will be prepared in hospital’s pharmacy. GT005 is supplied as part of a treatment kit
which includes a single GT005 vial, a diluent vial and an empty administration vial placed in a
labelled secondary container carton. The outer secondary carton will always remain with the
administration vial. The hospital pharmacy, or equivalent, will receive the product and diluent
according to local procedures. Storage will be at or below -60°C until requested for administration
in a facility with restricted access until it is released for patient administration. The investigator,
or designee, will ensure that the IMP is stored, prepared and dispensed by qualified staff members
designated as unmasked. Maximum storage duration will be until the end of September 2024.
_________________________
11
In case of applications submitted to Austria, Belgium, Croatia, Czech Republic, Denmark, Finland,
France, Ireland, Italy, the Netherlands and Spain, the applicant should specify if the dose is being
prepared in the hospital pharmacy. If the clinical dose is prepared at a location other than the hospital
pharmacy, this should be explained.

22
3.4. Logistics for on-site transportation of the clinical vector.
The applicant should provide information about the logistics for in-house transportation (i.e.
transfer of the clinical vector from storage to the administration site and –where applicable- site
where dose is prepared). The applicant should provide information about the characteristics of
the containers used addressing also disinfection procedures applied and labelling of the
containers.
GT005 will be transported to the operating theatre at ambient temperature and in accordance with
GMO requirements and/or local hospital procedures.
Frozen, thawed or diluted (in the
administration vial) GT005 will preferably be transported indoors. The IMP may only be transported
outdoors or in the locked Loading Syringe upon approval by Gyroscope and in adherence to
institutional procedures, in particular those related to the management of genetically modified (GM)
products. In summary:
a. Where IMP preparation and dilution is to be performed in the pharmacy – (for IMP storage
and administration in the same building): The Treatment Kit containing the frozen or thawed
IMP or diluted IMP (in the administration vial) or diluted IMP within the Loading Syringe can
be transported indoors. The filled and labelled administration vial will be enclosed in an
outer secondary carton for transfer to the operating theatre. The outer secondary carton
will always remain with the administration vial. Once the vial seal is broken, the vial will not
be transported outside the building.
b. Where IMP preparation and dilution is to be performed in the pharmacy (IMP storage and
administration are not in the same building but may be transported from one building to
another): The Treatment Kit containing the frozen or thawed IMP or diluted IMP (in the
administration vial) or diluted IMP within the Loading Syringe can be transported outdoors
from one building to another.
The Treatment Kit will be placed into a leak proof secondary container and sealed before placing it
into an insulated IMP transport container for frozen transport. The outer container will also be
labelled indicating the contents as a Risk Group 1 GMO investigational product in accordance with
local and regional regulatory requirements.
The locked and labelled Loading Syringe containing the IMP will be enclosed in a primary leakproof
sealable container and then placed in a secondary ambient temperature transport container for
transfer from the Pharmacy via the agreed route to the masked surgical team.
3.5. Information about reconstitution, finished medicinal product and
administration to patients.
Reconstitution (where
applicable,
summarise reconstitution steps):
For EXPLORE:
GT005 will be assessed at two dose levels (Low dose: 2E10 vg
and High dose: 2E11 vg). Dilution of GT005 is not required for

23
the high dose (2E11 vg), and for the lower dose, the dilution
will be made with dilution buffer provided in the IMP kit.
For HORIZON:
GT005 will be assessed at two dose levels (Medium dose: 5E10
vg and High dose: 2E11 vg) Dilution of GT005 is not required
for the high dose (2E11 vg). and for the lower dose, the
dilution will be made with dilution buffer provided in the IMP
kit.
Further details of preparation and dilution
are considered
confidential and are provided in a separate document (Annex
1 to the Common Application Form – Confidential
Information)
Pharmaceutical form
and strength:
Pharmaceutical Form: Suspension for injection
Strengths: 2E10 vg, 5E10 vg and 2E11 vg
Mode of administration:
Sub-retinal injection
Information on dosing and
administration schedule (in case
of repeated dosing):
Single dose
Information on
concomitant medication
that may affect the
shedding of the clinical
vector/ environmental
risks (e.g. administration
of laxatives,
administration of a
medicinal product that
could enhance the
replication activity of the
clinical vector,
administration of a
plasmid- based medicinal
product):
Not applicable
3.6 Measures to prevent dissemination into the environment.
a) Control measures during reconstitution (if applicable), handling and administration.

24
The individual preparing the dilution must use appropriate aseptic technique while preparing the
IMP. The appropriate personal protection equipment (PPE) (laboratory coat, safety glasses and
gloves etc.), clean air and single use instruments in theatres should be used to minimise the risk of
contamination.
IMP must be prepared in a designated aseptic preparation area that is not adjacent to potential
sources of contamination, including sinks or other water sources. The IMP preparation area should
be cleaned and disinfected with viricidal disinfectant. This includes both prior to, and following
preparation of the IMP, and any time there is evidence of soiling.
b) Personal protective equipment.
Laboratory coat, safety glasses and gloves.
c) Decontamination/cleaning measures after administration or in the case of accidental
spilling (i.e. decontamination /cleaning measures of potentially contaminated
materials, surfaces and areas). In addition, the disinfection procedures applied should
be justified by providing evidence that the chosen method is sufficiently active against
the clinical vector.
The nature of the waste generated includes used syringes, ancillary components, personal
equipment, needles, etc. used in dose preparation and administration and components used for
collecting body fluids samples after administration. It is anticipated that no more than 50 mL of
product (GT005) waste will be generated in the whole EXPLORE study, and no more than 120 mL of
product waste is expected to be generated in the whole HORIZON study.
Any disposable consumables/instruments used during the handling, dose preparation and
administration procedures, including syringes and needles used for the dilution of the IMP, will be
disposed of according to local procedures in a manner consistent with the standard practice of the
institution for Risk Group 1 GMOs. In the medical facility, this will involve containment in sharps bins
or clearly marked bags (e.g. biohazard, medical waste) prior to autoclaving and/or incineration either
on or off site as per local institutional guidelines.
Non-
disposable instruments such as the plastic trays that have been used during the dose
preparation and administration procedures and have potentially come into contact with GT005, will
be sprayed with a viricidal disinfectant in accordance with local guidelines and institutional
procedures related to the management of Risk Group 1 GMOs. Any materials used for cleaning (e.g.
paper towel or other solid waste such as biobins will be disposed of following local waste procedures
for Risk Group 1 GMOs. Alternatively, any solid waste including sharps containers maybe autoclaved
to inactivate the GMO waste. Other waste, such as PPE and injection connection tubing, which is not
routinely exposed to vector and is therefore of low risk, will be disposed of according to local
procedures for medical waste.

25
Where permitted, contaminated liquids will be disposed of as specific waste or by decontamination
with a detergent-based viricidal disinfectant as per local guidelines and institutional procedures and
according to the manufacturer’s instructions.
Decontamination and liquid waste Treatment
Spill: The spill will be contained, and the area will be decontaminated using a viricidal disinfectant as
per local guidelines and institutional procedures and according to the manufacturer’s instructions.
A spill kit will be available at all times during all the steps, but minimally during the preparation and
administration procedure. Details are given in the Pharmacy Manual, describing the handling of the
IMP in the pharmacy and the administration procedures that will be handed over to the site during
the site initiation visit (prior to starting the study).
Liquid waste Disposal: Contami
nated liquids will be disposed of as specific waste or by
decontamination with viricidal disinfectant as per local guidelines and institutional procedures and
according to the manufacturer’s instructions followed by disposal in a sink, using plenty of water to
flush. Alternatively, contaminated liquids and viral stock can be disposed of as biohazardous waste.
d) Elimination or inactivation of left-overs of the finished product at the end of the clinical
trial.
Any opened and/or unopened GT005, and/or expired Treatment Kits, diluent vials (used and unused)
and administration vials used during the preparation and administration of GT005 will be destroyed
on site (once directed by the unmasked CRA), according to local procedures in a manner consistent
with the standard practice of the institution for Risk Group 1 GMOs. In the medical facility, this will
involve temporary containment in sharps bins or clearly marked bags (e.g. biohazard, medical waste)
prior to autoclaving and/or incineration either on or off site.
Records of the receipt and dispensing of the IMP will be kept by the site (pharmacy/storage unit) to
provide complete accountability of all used and unused IMP.
e) Waste treatment (including also –where applicable- decontamination and
disposal of potentially contaminated waste that accumulates outside the clinical
trial site). Where applicable, identify also the company responsible for waste
management.
In the medical facility, this will involve temporary containment in sharps bins or clearly marked bags
(e.g. biohazard, medical waste) prior to autoclaving and/or incineration either on or off site.
The waste is removed from site by a 3
rd
party vendor approved by the clinical facility.
f) Recommendations given to clinical trial subjects to prevent dissemination
(where applicable).
Advice given on contraception provided below in i) Other measures (where applicable).

26
g) Recommendations on donation of blood/cells/tissues/organs by the
clinical trial subject.
The eye is an immune privileged organ [Medawar, 1948] and there is minimal dissemination of the
vector outside of the ocular space [Wu et al., 2011]. This has been demonstrated in GT005 non-
clinical studies where biodistribution studies showed that GT005 vector was detected at high levels
at the dosing site (retina, RPE and choroid), relatively moderate levels outside the dosing site and
in vitreous humour, and at low levels in the spleen and the optic tract/nerve/chiasm at Week 26
post dosing. No GT005 vector was detected in heart, kidney, liver, lung, ovary, and testes samples.
The non-clinical data suggested that subretinal administration of GT005 results in minimal
dissemination of the vector outside of the ocular space which is consistent with published
literature on AAV2-gene therapies administered into the eye, with signals falling over time and the
dosing site yielding the highest average vector concentrations compared to the other tissues
analysed.
In addition, interim clinical assessment of vector shedding by Gyroscope Therapeutics in the Phase
I/II FOCUS clinical study shows that vector is expected to be cleared (no further shedding) locally
and systemically from patients within week 1 of treatment. This was also consistent with other
data presented by other published studies (Luxturna, FDA, 2017; EPAR, EMEA/H/C/004451-
IB/0011/G). Therefore, the risks of vector transmission from organ donation post-GT005 treatment
are considered extremely minimal. This includes corneal donation since GT005 is administered
directly into the subretinal space at the back of the eye.
The European Commission Good Practice on the assessment of GMO related aspects in the context
of clinical trials with AAV clinical vectors (European Commission; Advanced Therapies access date:
21 Feb 2022) also considers that ‘the non-pathogenic nature of AAVs and the limited quantitative
exposure, the risk associated with the possibility of latent infection in non-target individuals who
receive blood, cells, tissues or organs from a patient treated with an AAV clinical vector is
considered negligible’.
In light of the above, and with appreciation of the importance of organ donation in conjunction with
understanding that the rules regarding organ donation may differ across different
jurisdictions/territories, the Sponsor has taken the position not to provide any specific restrictions
or recommendations on organ donation post-GT005 treatment. The decision is left to the subject, in
consultation with the investigator and/or primary care provider, as appropriate.
i) Other measures (where applicable).
Women of child-bearing potential must have a negative pregnancy test within 2 weeks prior to
randomisation. A pregnancy test is not required for postmenopausal women (defined as being at
least 12 consecutive months without menses) or those surgically sterilised (those having a
bilateral tubal ligation/bilateral salpingectomy, bilateral tubal occlusive procedure, hysterectomy,
or bilateral oophorectomy).
Females of child-bearing potential (not surgically sterile or 2 years postmenopausal) are required
to use two methods of contraception (one of which being a barrier method) and must agree to

27
continue to use these methods of contraception for 90 days post-dosing. Acceptable methods of
contraception include barrier method with spermicide, intrauterine device, or steroidal
contraceptive (oral, transdermal, implanted, and injected) in conjunction with a barrier method
or abstinence. True abstinence is defined when this is in line with the preferred and usual lifestyle
of the subject. Periodic abstinence (e.g. calendar, ovulation, symptothermal, post-ovulation
methods) and withdrawal are not acceptable methods of contraception.
Male subjects who have female partners of child-bearing potential, should, with their partner,
use a barrier method in conjunction with a second method of contraception for 90 days post-
dosing.
The 90 day window was determined from the NHP data showing that vector shedding in saliva
samples was below the limit of detection at Week 4, and in tear and blood samples at Week 13.
3.7. Sampling and further analyses of samples from study subjects
This Section should be filled in where samples are being taken from patients which may contain
GMOs in the context of the clinical trial and the application is submitted to the following
jurisdictions: Croatia, Czech Republic, Germany, Ireland, the Netherlands, Spain
a) Describe how samples will be handled/stored/transported.
To the extent that handling/ storage and transport of samples are treated under same
procedures as the clinical vector, cross-reference can be made as appropriate.
Patient Sampling: Processing, Analysis and Storage: Biosampling will be performed regularly for
study purposes, and as needed for routine patient care purposes.
Sampling will be performed within the hospital and all samples will be labelled as per local hospital
procedures. Sampling and transportation of samples, as well as their processing and/or storage
within the clinical study site will not require additional precautionary or containment measures.
Sample handling and transportation of patient samples within the hospital will be done per local
hospital procedures. For all human samples, routine precautions, designed to contain pathogens in
blood and to protect the hospital staff from pathogens in blood, will be taken. These precautions
include the use of gloves and a laboratory coat, gown, or uniform. No further restrictions will be
applied in addition to these routine precautionary measures that will be in accordance with local
hospital procedures for handling human samples. After sampling the waste will be processed as
hospital specific waste.
b) Indicate whether and at which time points samples that may contain the administered
clinical vector are taken from study subjects.
Observation of subjects will be by means of post-administration surveillance. Subjects will be
followed-up for 96 weeks post-dosing. After the final follow-up visit, all subjects will be enrolled
into a dedicated clinical trial for a 5 year long-term follow-up period.

28
c) If samples are stored at the clinical site, describe storage location and storage conditions.
Patient samples are stored at 4° C in a dedicated fridge for a maximum of two weeks prior to
shipping to an analysis site in the Netherlands.
d) Explain if there is any non-routine
12
testing of the samples and indicate whether the
clinical vector is generated de novo during the testing.
No non-routine testing will occur.
12
Standard clinical care tests as well as tests required to fulfil long-term follow-up of clinical trial subjects need not be mentioned.

29
SECTION 4 – OTHER DATA REQUIREMENTS
4.1. Plan of the site(s) concerned
Applicants should provide a copy of the plan of the site where the clinical trial takes place
if the application is submitted to the following jurisdictions: Austria, Belgium, Croatia,
Czech Republic, Finland, France, Hungary, Ireland and Italy.
Whitfield surgical site plan provided as part of submission package.
30
4.2 Other information
Submissions to Austria:
In addition to the plan of the site, a description of the location of the autoclave should be
provided –as appropriate- as part of the description of the measures to prevent dissemination
into the environment referred in Section 3.6 (d) and (e).
Submissions to Belgium:
In addition to the plan of the site, a description of the location of the autoclave and the
biosafety cabinet should be provided –as appropriate- as part of the description of the
measures to prevent dissemination into the environment referred in Section 3.6 (d) and (e).
The applicant is also asked to provide an overview (table) of the rooms involved in the CT
activity by indicating for each of those the number of the room, the type of handling carried out
(e.g. storage, administration of the IMP, reconstitution of the IMP) and the containment level.
Submissions to Czech Republic:
In addition to the plan of the site, a description of the location of the autoclave should be
provided –as appropriate- as part of the description of the measures to prevent dissemination
into the environment referred in Section 3.6 (d) and (e).
Submissions to Denmark:
The applicant should explain if left-overs are stored at the clinical site and, if in the
affirmative, for how long as part of the information submitted in Section 3(6)(d).
The applicant should provide the following information on waste treatment in Section
3(6)(e):
− Whether and for how long the waste will be stored (or frequency of waste disposal),
− Storage location,
− Logistics for on-site transportation of the waste (similar as asked for the clinical vector in
Section 3.4), and
− In case of chemical decontamination whether the chosen disinfectant and method is
sufficiently active against the clinical vector (similar as in Section 3.6.c)
Submissions to France:
The plan of the site should indicate clearly the location of a PSMII, or an equivalent device.
Submissions to Germany:
The applicant is not required to provide further information in Section 3(6)(c) if he/she
confirms that the disinfectant and decontamination procedure are included in the list
of the Robert Koch Institute of currently approved disinfectants and disinfectant
procedures or the VAH (Verbund für Angewandte Hygiene e.V) list of disinfectants.
The applicant should explain if left-overs are stored at the clinical site and, if in the
31
affirmative, for how long as part of the information submitted in Section 3(6)(d).
The applicant should provide the following information on waste treatment in Section
3(6)(e):
− Whether and for how long the waste will be stored (or frequency of waste disposal),
− Storage location,
− Logistics for on-site transportation of the waste (similar as asked for the clinical vector in
Section 3.4), and
− In case of chemical decontamination whether the chosen disinfectant and method is
sufficiently active against the clinical vector (similar as in Section 3.6.c)
If samples are stored at the clinical site, the maximum duration of the storage should
be stated in Section 3.7 (c).
The applicants is required to provide emergency response plans.
Submissions to Ireland:
In addition to the plan of the site, a description of the location of the autoclave should
be provided –as appropriate- as part of the description of the measures to prevent
dissemination into the environment referred in Section 3.6 (d) and (e).
If samples are stored at the clinical site, the maximum duration of the storage should
be stated in Section 3.7(c).
Submissions to Italy:
In addition to the plan of the site, a description of the location of the autoclave should
be provided –as appropriate- as part of the description of the measures to prevent
dissemination into the environment referred in Section 3.6 (d) and (e).
If the manufacturer of the clinical vector is located in Italy, the authorisation issued to
the premises should be declared in Section 1.3.
SECTION 5- ENVIRONMENTAL RISK ASSESSMENT
Specific environmental risk assessment
Considering the specific characteristics of the investigational medicinal product (as described
in Section 2 of the application form), the applicant considers that the specific environmental
risk assessment provided for in Section 2 of the Good Practice on the assessment of GMO
related aspects in the context of clinical trials with AAV clinical vectors is applicable:
Yes
x
No □ If the answer to the above is NO, the following information should be provided:
• For submissions made under Directive 2001/18/EC: an environmental risk assessment
is required in accordance with Annex II thereof.
• For submissions made under Directive 2009/41/EC: an assessment of the risks to
human health and the environment in accordance with Article 4 thereof.
