
©Institute for Clinical and Economic Review, 2022
Medications for Obesity Management:
Effectiveness and Value
Evidence Report
August 31, 2022
Prepared for

©Institute for Clinical and Economic Review, 2022 Page i
Evidence Report – Medications for Obesity Management
ICER Staff and Consultants
University of Illinois at Chicago Modeling Group
Steven J. Atlas, MD, MPH
Associate Professor of Medicine
Harvard Medical School
Director of Practice-Based Research and Quality
Improvement
Division of General Internal Medicine
Massachusetts General Hospital
Molly Beinfeld, MPH
(Former) Senior Research Lead, Evidence Synthesis
Institute for Clinical and Economic Review
Victoria Lancaster, PharmD, MSc, MBA
Health Technology Assessment Fellow
Institute for Clinical and Economic Review
Emily Nhan
Research Assistant
Institute for Clinical and Economic Review
Ashton Moradi, PharmD, MS
Health Economist
Institute for Clinical and Economic Review
David M. Rind, MD, MSc
Chief Medical Officer
Institute for Clinical and Economic Review
Steven D. Pearson, MD, MSc
President
Institute for Clinical and Economic Review
Francesca L. Beaudoin, MD, PhD, MS
Senior Medical Advisor
Institute for Clinical and Economic Review
Kibum Kim, PhD
Assistant Professor
University of Illinois at Chicago
Pei-Wen (Hilary) Lien, MSc
PhD Candidate
University of Illinois at Chicago
Kanya Shah, PharmD, MS, MBA
PhD Candidate
University of Illinois at Chicago
Daniel R. Touchette, PharmD, MA
Professor, University of Illinois at Chicago
Director, Center for Pharmacoepidemiology and
Pharmacoeconomic Research
The role of the University of Illinois at Chicago is
limited to the development of the cost-effectiveness
model, and the resulting ICER report does not
necessarily represent the views of the University of
Illinois at Chicago.
None of the above authors disclosed any conflicts of interest defined as more than $10,000 in health care company
stock or more than $5,000 in honoraria or consultancies relevant to this report during the previous year from
health care manufacturers or insurers.
DATE OF
PUBLICATION: August 31, 2022
How to cite this document: Atlas SJ, Kim K, Beinfeld M, Lancaster V, Nhan E, Lien PW, Shah K, Touchette DR,
Moradi A, Rind DM, Pearson SD, Beaudoin, FL. Medications for Obesity Management: Effectiveness and Value;
Evidence Report. Institute for Clinical and Economic Review, August 31, 2022.
https://icer.org/assessment/obesity-
management-2022/.
Steven J. Atlas served as the lead author for the Report. Molly Beinfeld led the systematic review and authorship
of the comparative clinical effectiveness section of this Report in collaboration with Victoria Lancaster and Emily

©Institute for Clinical and Economic Review, 2022 Page ii
Evidence Report – Medications for Obesity Management
Nhan. Kibum Kim developed the cost-effectiveness model and authored the corresponding sections of the Report
with assistance from Daniel R. Touchette, Pei-Wen Lien, and Kanya Shah. Development of the cost-effectiveness
model was also assisted by Jessica Benitez-Burke and Lauren Lee. Ashton Moradi provided consultation on the
cost-effectiveness analyses and developed the budget impact model. Francesca Beaudoin, David M. Rind, and
Steven D. Pearson provided methodologic guidance on the clinical and economic evaluations. We would also like
to thank Laura Cianciolo, Monica Frederick, and Foluso Agboola for their contributions to this Report.

©Institute for Clinical and Economic Review, 2022 Page iii
Evidence Report – Medications for Obesity Management
About ICER
The Institute for Clinical and Economic Review (ICER) is an independent non-profit research organization that
evaluates medical evidence and convenes public deliberative bodies to help stakeholders interpret and apply
evidence to improve patient outcomes and control costs. Through all its work, ICER seeks to help create a future in
which collaborative efforts to move evidence into action provide the foundation for a more effective, efficient, and
just health care system. More information about ICER is available at https://icer.org/
.
The funding for this report comes from government grants and non-profit foundations, with the largest single
funder being the Arnold Ventures. No funding for this work comes from health insurers, pharmacy benefit
managers, or life science companies. ICER receives approximately 29% of its overall revenue from these
health industry organizations to run a separate Policy Summit program, with funding approximately equally split
between insurers/PBMs and life science companies. There are no life science companies relevant to this review
who participate in this program. For a complete list of funders and for more information on ICER's support, please
visit https://icer.org/who-we-are/independent-funding/
.
For drug topics, in addition to receiving recommendations from the public
, ICER scans publicly available
information and also benefits from a collaboration with IPD Analytics, an independent organization that performs
analyses of the emerging drug pipeline for a diverse group of industry stakeholders, including payers,
pharmaceutical manufacturers, providers, and wholesalers. IPD provides a tailored report on the drug pipeline on
a courtesy basis to ICER but does not prioritize topics for specific ICER assessments.
About New England CEPAC
The New England Comparative Effectiveness Public Advisory Council (CEPAC) – a core program of ICER – provides a
public venue in which the evidence on the effectiveness and value of health care services can be discussed with
the input of all stakeholders. New England CEPAC seeks to help patients, clinicians, insurers, and policymakers
interpret and use evidence to improve the quality and value of health care.
New England CEPAC is an independent committee of medical evidence experts from across New England, with a
mix of practicing clinicians, methodologists, and leaders in patient engagement and advocacy. All council members
meet strict conflict of interest guidelines and are convened to discuss the evidence summarized in ICER reports and
vote on the comparative clinical effectiveness and value of medical interventions. More information about New
England CEPAC is available at
https://icer.org/who-we-are/people/independent-appraisal-committees/new-
england-cepac/.
The findings contained within this Report are current as of the date of publication. Readers should be aware that
new evidence may emerge following the publication of this Report that could potentially influence the results.
ICER may revisit its analyses in a formal update to this report in the future.
The economic models used in ICER Reports are intended to compare the clinical outcomes, expected costs, and
cost-effectiveness of different care pathways for broad groups of patients. Model results therefore represent
average findings across patients and should not be presumed to represent the clinical or cost outcomes for any
specific patient. In addition, data inputs to ICER models often come from clinical trials; patients in these trials may
differ in real-world practice settings.

©Institute for Clinical and Economic Review, 2022 Page iv
Evidence Report – Medications for Obesity Management
In the development of this report, ICER’s researchers consulted with several clinical experts, patients,
manufacturers, and other stakeholders. The following experts provided input that helped guide the
ICER team as we shaped our scope and report. It is possible that expert reviewers may not have had
the opportunity to review all portions of this revised Evidence Report. None of these individuals is
responsible for the final contents of this report, nor should it be assumed that they support any part
of it. The report should be viewed as attributable solely to the ICER team and its affiliated
researchers.
For a complete list of stakeholders from whom we requested input, please visit:
https://icer.org/wp-content/uploads/2022/03/ICER_Obesity_Stakeholder-List_030322.pdf
Expert Reviewers
Harold Bays, MD, FOMA, FTOS, FACC, FNLA, FASPC
Medical Director and President
Louisville Metabolic and Atherosclerosis Research Center
Clinical Associate Professor
University of Louisville School of Medicine
Louisville Metabolic and Atherosclerosis Research Center has received research grants from
Allergan, Alon Medtech/Epitomee, Altimmune, Amgen, Boehringer Ingelheim, Eli Lilly, Novartis,
NovoNordisk, Pfizer, and Vivus. Dr. Bays has served as a consultant/advisor for Altimmune, Amgen,
and Boehringer Ingelheim.
Joseph Nadglowski, Jr.
President and Chief Executive Officer
Obesity Action Coalition
Joseph Nadglowski, Jr. has no personal financial relationships with any obesity-related industry. He
is an employee of the Obesity Action Coalition (OAC) and OAC does receive funding from a wide-
variety of obesity related industry including those providing behavioral, pharmaceutical, device, and
surgical interventions.
Fatima Cody Stanford, MD, MPH, MPA, MBA, FAAP, FACP, FAHA, FAMWA, FTOS
Associate Professor of Medicine and Pediatrics
Obesity Medicine Physician Scientist
Equity Director, Massachusetts General Hospital Endocrine Division
Massachusetts General Hospital and Harvard Medical School
Dr. Stanford has received consulting fees and/or honoraria from Novo Nordisk, Eli Lilly, Boehringer
Ingelheim, GoodRX, Calibrate, and Coral Health.

©Institute for Clinical and Economic Review, 2022 Page v
Evidence Report – Medications for Obesity Management
Table of Contents
Executive Summary ............................................................................................................................ ES1
1. Background ........................................................................................................................................ 1
2. Patient and Caregiver Perspectives ................................................................................................... 4
3. Comparative Clinical Effectiveness .................................................................................................... 6
3.1. Methods Overview ...................................................................................................................... 6
Scope of Review ............................................................................................................................. 6
Evidence Base ................................................................................................................................ 6
3.2. Results ....................................................................................................................................... 13
Clinical Benefits ............................................................................................................................ 13
Harms ........................................................................................................................................... 24
Subgroup Analyses and Heterogeneity ........................................................................................ 33
Uncertainty and Controversies .................................................................................................... 33
3.3. Summary and Comment ........................................................................................................... 36
4. Long-Term Cost Effectiveness .......................................................................................................... 40
4.1. Methods Overview .................................................................................................................... 40
Scenario Analyses......................................................................................................................... 43
4.2. Key Model Assumptions and Inputs ......................................................................................... 44
Model Assumptions ..................................................................................................................... 44
4.3. Results ....................................................................................................................................... 49
Base-Case Results......................................................................................................................... 49
Sensitivity Analyses ...................................................................................................................... 50
Scenario Analyses......................................................................................................................... 51
Threshold Analyses ...................................................................................................................... 53
Model Validation .......................................................................................................................... 53
Uncertainty and Controversies .................................................................................................... 54
4.4. Summary and Comment ........................................................................................................... 56
5. Contextual Considerations and Potential Other Benefits ................................................................ 57
6. Health-Benefit Price Benchmarks .................................................................................................... 59
7. Potential Budget Impact .................................................................................................................. 60

©Institute for Clinical and Economic Review, 2022 Page vi
Evidence Report – Medications for Obesity Management
7.1. Overview of Key Assumptions .................................................................................................. 60
7.2. Results ....................................................................................................................................... 61
References ........................................................................................................................................... 62
Supplemental Materials
A. Background: Supplemental Information .........................................................................................A1
A1. Definitions ..................................................................................................................................A1
A2. Potential Cost-Saving Measures in Obesity Management ........................................................A2
A3. Future Therapies ........................................................................................................................A2
B. Patient Perspectives: Supplemental Information ............................................................................ B1
B1. Methods ..................................................................................................................................... B1
C. Clinical Guidelines ............................................................................................................................ C1
Veterans’ Health Administration/Department of Defense.......................................................... C1
Canadian Clinical Practice Guideline ............................................................................................ C1
Endocrine Society ......................................................................................................................... C2
National Institute for Health and Care Excellence (NICE) ............................................................ C3
D. Comparative Clinical Effectiveness: Supplemental Information .................................................... D1
D1. Detailed Methods ..................................................................................................................... D1
PICOTS ......................................................................................................................................... D1
Data Sources and Searches ......................................................................................................... D5
Study Selection ............................................................................................................................ D9
Data Extraction and Quality Assessment .................................................................................... D9
Assessment of Level of Certainty in Evidence .......................................................................... D10
Assessment of Bias .................................................................................................................... D10
Data Synthesis and Statistical Analyses .................................................................................... D10
Supplemental NMA Methods ................................................................................................... D10
Supplemental NMA Results ...................................................................................................... D11
D2. Additional Clinical Evidence .................................................................................................... D16
Evidence Base ........................................................................................................................... D16
Results ....................................................................................................................................... D20
Harms ........................................................................................................................................ D35

©Institute for Clinical and Economic Review, 2022 Page vii
Evidence Report – Medications for Obesity Management
D3. Evidence Tables ...................................................................................................................... D39
D4. Ongoing Studies ...................................................................................................................... D83
D5. Previous Systematic Reviews and Technology Assessments ................................................. D89
E. Long-Term Cost-Effectiveness: Supplemental Information ............................................................. E1
E1. Methods ..................................................................................................................................... E1
Rationale for Not Including Certain Health States in the Base Case ........................................... E1
Impact Inventory .......................................................................................................................... E1
Description of evLY Calculations .................................................................................................. E3
Target Population......................................................................................................................... E3
Treatment Strategies ................................................................................................................... E4
E2. Model Inputs and Assumptions ................................................................................................. E4
Model Inputs ................................................................................................................................ E5
E3. Results ........................................................................................................................................ E9
Cost-Effectiveness Plane .............................................................................................................. E9
Undiscounted Base-Case Results ............................................................................................... E10
Cumulative Incidence of Cardiovascular Conditions and Mortality .......................................... E11
E4. Sensitivity Analyses .................................................................................................................. E13
One-Way Sensitivity Analysis ..................................................................................................... E13
Probabilistic Sensitivity Analysis ................................................................................................ E16
E5. Scenario Analyses ..................................................................................................................... E19
E6. Heterogeneity and Subgroups ................................................................................................. E22
E7. Prior Economic Models ............................................................................................................ E23
F. Potential Budget Impact: Supplemental Information .................................................................... F25
Methods ..................................................................................................................................... F25
Results ........................................................................................................................................ F26

©Institute for Clinical and Economic Review, 2022 Page viii
Evidence Report – Medications for Obesity Management
List of Acronyms and Abbreviations Used in this Report
A1C Glycated hemoglobin
ACC American College of Cardiology
AHA American Heart Association
AHRQ Agency for Healthcare Research and Quality
BMI Body mass index
CI Confidence interval
CPAP Continuous positive airway pressure
dL Deciliter
evLY Equal-value life year
FDA Food and Drug Administration
GLP-1 Glucagon-like peptide-1
GIP Glucose-dependent insulinotropic polypeptide
HRQoL Health-related quality of life
IBT Intensive behavioral therapy
IDS-SR Inventory of Depressive Symptomatology Self-Report
IWQOL Impact of Weight on Quality of Life
kg Kilogram
LDL Low density lipoprotein
m Meters
MCS Mental component summary
mg Milligram
mmHg Millimeter of mercury
mmol/L Millimoles per liter
n number
N Total number
NMA Network meta-analysis
PCS Physical component summary
PHQ-9 Patient Health Questionnaire
QALY Quality-adjusted life year
SBP Systolic blood pressure
US United States
USPSTF United States Preventive Services Task Force
WAC Wholesale acquisition cost

©Institute for Clinical and Economic Review, 2022 Page ES1
Evidence Report – Medications for Obesity Management Return to Table of Contents
Executive Summary
Obesity is a common chronic disease that increases the risk of other conditions such as diabetes
mellitus, cancer, and heart disease as well as death.
1,2
Individuals with overweight and obesity also
face considerable social stigma that can have both direct (e.g., mental health, wellbeing) and
indirect consequences (e.g., engagement with health care providers).
3
Body mass index (BMI,
weight in kilograms/height in meters
2
) is commonly used to assess for obesity because it is easy to
measure and correlates with body fat measurements.
4,5
In 2015, the number of adults in the
United States (US) with overweight or obesity was estimated to be 79 million and 70 million,
respectively.
6,7
The prevalence of obesity surpassed 40% of US adults in 2018,
8
but among some
racial and ethnic groups obesity is even more prevalent with higher proportions for Hispanic adults
and highest proportions among non-Hispanic Black women.
9,10
The direct medical costs
attributable to obesity are staggering, estimated to be $260 billion in the US in 2016.
11
Given the
high of obesity and its many adverse clinical and cost consequences, cost-effective treatments for
this chronic condition are imperative.
Interest in medications to reduce weight and improve health in individuals with obesity has
increased due to more non-surgical alternatives and data suggesting that newer medications have
an acceptable safety profile and may be more effective in promoting weight loss. Limitations of
medications for weight loss include side effects that lead to patient discontinuation, and weight
regain when stopped. Under a chronic disease framework, clinical experts concluded that long-
term anti-obesity medication use would likely be needed, particularly to prevent complications of
obesity such as heart disease. This Report reviews four medications approved by the US Food and
Drug Administration (FDA): semaglutide (Wegovy®, Novo Nordisk, June 2021), liraglutide (Saxenda®,
Novo Nordisk, 2014), phentermine/topiramate (Qysmia®, Vivus, 2012), and bupropion/naltrexone
(Contrave®, Currax Pharmaceuticals, 2014). Semaglutide and liraglutide are glucagon-like peptide-1
(GLP-1) receptor agonists that are also approved for diabetes mellitus and given by subcutaneous
injection, whereas phentermine/topiramate and bupropion/naltrexone are combination oral agents
that work via other mechanisms. Other promising therapies (e.g., tirzepatide) are still under
investigation and are therefore not included in the scope of this review.
12
For adults without pre-existing diabetes mellitus and either a BMI ≥30 kg/m
2
or ≥27 kg/m
2
with at
least one weight-related comorbid condition (such as hypertension or dyslipidemia), the four
interventions added to usual care all reduced body weight compared to usual care alone, which
included standard diet and activity and lifestyle recommendations. Indirect mean and categorical
weight loss reduction comparisons across the drugs as well as direct head-to-head evidence
between two of the agents (semaglutide and liraglutide) suggest that semaglutide and
phentermine/topiramate achieve greater weight loss than liraglutide and bupropion/naltrexone.
Semaglutide and liraglutide improved blood sugar and blood pressure compared to usual care, but

©Institute for Clinical and Economic Review, 2022 Page ES2
Evidence Report – Medications for Obesity Management Return to Table of Contents
how they compare to phentermine/topiramate and bupropion/naltrexone is less certain. In
addition, none of these drugs have assessed long-term outcomes in adults without pre-existing
diabetes mellitus, and thus there is uncertainty around long-term benefits such as cardiovascular
morbidity and mortality. Adverse events were common among all interventions, but few serious
harms were noted. All interventions had greater discontinuation due to adverse events than for
placebo, though semaglutide appears to have lower rates than the other drugs. For all
interventions, there is uncertainty about whether sustained weight loss leads to decreased clinical
endpoints, and if weight regain occurs over time despite continued therapy.
Given the strength of the evidence on weight loss outcomes in the trials and uncertainty around
long-term outcomes for adults without pre-existing diabetes mellitus and with obesity or
overweight with at least one comorbid condition, Table ES1 presents the ICER evidence ratings
comparing each intervention with lifestyle modification to lifestyle modification alone and
comparing semaglutide and the other interventions with lifestyle modification.
Table ES1. Evidence Ratings for Treatment of Adults with Obesity
Treatment
Comparator
Evidence Rating
Semaglutide
Lifestyle modification
B+
Liraglutide
Lifestyle modification
B
Phentermine/Topiramate
Lifestyle modification
C++
Bupropion/Naltrexone
Lifestyle modification
C+
Semaglutide
Liraglutide
C+
Phentermine/topiramate
C+
Bupropion/naltrexone
C++
Information about ICER’s Evidence Rating Matrix may be found here.
At current prices and with commonly accepted cost-effectiveness benchmarks, results suggest that
phentermine/topiramate in addition to lifestyle modification is cost effective compared with
lifestyle modification alone. The cost effectiveness of treatment of obesity with semaglutide or
liraglutide in patients without diabetes mellitus exceeds commonly used thresholds.
Bupropion/naltrexone is cost effective only at higher thresholds (see Table 4.5
).
The health-benefit price benchmark for semaglutide is $7,500 to $9,800 per year; this would require
a discount from the wholesale acquisition cost of 44-57%.
In summary, among the agents we reviewed, greater weight loss was seen with semaglutide and
with phentermine/topiramate; less weight loss was seen with liraglutide and with
bupropion/naltrexone. Although few serious harms were noted for all the interventions,
semaglutide may have lower rates of discontinuation and, along with liraglutide, may have
additional cardiovascular benefits that extend beyond weight loss effects. Phentermine/topiramate
is substantially less expensive than semaglutide and liraglutide, meets commonly accepted cost-
effectiveness thresholds and is actually cost-saving when prescribed generically.

©Institute for Clinical and Economic Review, 2022 Page ES3
Evidence Report – Medications for Obesity Management Return to Table of Contents
Bupropion/naltrexone is cost effective only at higher thresholds, but is cost effective when
prescribed generically. Semaglutide requires substantial discounts from the wholesale acquisition
cost to meet typical thresholds, but it is more effective, less burdensome, and more cost effective
than liraglutide.

©Institute for Clinical and Economic Review, 2022 Page 1
Evidence Report – Medications for Obesity Management Return to Table of Contents
1. Background
Obesity is a common chronic disease that increases the risk of other conditions such as diabetes
mellitus, hypertension, dyslipidemia, cancer, heart disease, and death.
1,2
Individuals with
overweight or obesity face a considerable social stigma that can make them feel judged, shamed,
and ostracized, and can affect interactions with family, friends, and even health professionals.
3
Because obesity can start in childhood, the stigma can affect social interactions, educational
development, relationships, and work.
5,13
The net effect is that obesity can have a profound impact
on all aspects of patients’ lives and those of their families and caregivers.
Obesity is defined by the World Health Organization as abnormal or excessive fat accumulation that
presents a risk to a person’s health.
14
While not optimal for assessing individuals with high or low
muscle mass, body mass index (BMI, weight in kilograms/height in meters
2
) is commonly used to
assess obesity because it is easy to reliably measure and correlates with body fat measurements.
4,5
More than two-thirds of the United States (US) population have overweight (BMI ≥25) or obesity
(BMI ≥30). The prevalence of obesity among adults has increased over time and was 40-45% in
2017-2018.
8,15
Among children and adolescents, the prevalence of obesity is almost 20%.
9
The
total number of adults with overweight was estimated at 79 million with another 70 million
estimated to have obesity in 2015, and with half the US population projected to have obesity by
2030.
6,7
The prevalence of obesity varies among racial and ethnic groups, being higher for Hispanic
adults and highest among non-Hispanic Black women.
9,10
Screening adults for obesity is
recommended by the US Preventive Services Task Force.
16
Given the prevalence of obesity and its
impact on health, the direct medical costs of obesity are staggering, estimated to be $260 billion in
the US in 2016.
11
The financial impact of obesity on individuals includes not only direct medical
costs but also indirect costs of lower wages and greater work loss and disability.
17,18
The stigma of obesity in society includes perceptions that attribute the problem to an individual’s
inability to control caloric intake and physical activity. However, it is recognized that energy
balance dysregulation is the result of interactions among complex genetic factors associated with
the body’s mechanisms that control energy balance and contribute to developing obesity.
19,20
An
individual’s lifestyle is also impacted by societal, economic, and cultural factors, which have
contributed to the rise in obesity. This complexity supports the idea that treating obesity and its
consequences must consider the potential range of causes that contribute to any one individual
with obesity.
The goal of therapy for obesity is to broadly prevent, treat, or reverse its complications, including its
impact on quality of life.
21,22
Patients cite a variety of reasons for wanting to lose weight including
improved health, self-esteem, and body image. Treatments to promote weight loss are intended to
improve health and prevent the health risks associated with obesity (e.g., diabetes, hypertension,
dyslipidemia, heart disease, cancer, fatty liver, osteoarthritis, sleep apnea) and ultimately improve

©Institute for Clinical and Economic Review, 2022 Page 2
Evidence Report – Medications for Obesity Management Return to Table of Contents
quality of life and longevity.
5,23
Observational studies support an association between weight loss
and reductions in mortality.
4
Initial weight loss treatments focus on lifestyle interventions that
variably combine healthful nutrition, increased physical activity, and behavioral modifications.
24,25
Though helpful for some, weight loss is usually modest and regaining weight over time occurs in the
vast majority of individuals. Earlier generation medications also had modest effects on weight loss,
and some were found to pose significant health risks. The introduction of surgical procedures to
promote weight loss demonstrated that, for severe obesity, significant weight loss was possible and
was associated with decreased weight-related complications.
26,27
This supports the notion that
successfully managing obesity as a chronic condition can lead to long-term health benefits.
For individuals who have not achieved desired weight loss with lifestyle changes, there are multiple
pharmacotherapy options indicated to promote weight loss and prevent complications of obesity.
Pharmacotherapy is often considered first-line before more invasive weight loss techniques are
considered (e.g., bariatric surgery). Currently, approved medications by the US Food and Drug
Administration (FDA) include the single agents: phentermine (1959), orlistat (Xenical®, H2 Pharma,
2007), liraglutide (Saxenda®, Novo Nordisk, 2014), and semaglutide (Wegovy®, Novo Nordisk, June
2021), and the combination drugs: phentermine/topiramate (Qysmia®, Vivus, 2012) and
bupropion/naltrexone (Contrave®, Currax Pharmaceuticals, 2014).
Semaglutide and liraglutide are glucagon-like peptide-1 (GLP-1) receptor agonists that are also
approved for diabetes mellitus due to their effect in stimulating insulin production. Their weight
loss effect is mediated in part by decreasing hunger and delaying gastric emptying.
19
Both are given
by subcutaneous injection with liraglutide administered daily and semaglutide weekly. The other
FDA-approved medications are administered by mouth and taken daily. Because orlistat results in
modest weight loss and causes intestinal side effects, it is less commonly used for initial medication
management and is not reviewed in this Report. Phentermine is an amphetamine-like medication
that suppresses appetite and is approved for short-term use (less than 12 weeks). It is also
available in combination with topiramate, a carbonic anhydrase inhibitor used to treat seizures.
The combination of bupropion and naltrexone works in the brain to decrease hunger.
19
Bupropion
is an inhibitor of norepinephrine and dopamine and is an antidepressant and anti-anxiety
medication. Naltrexone is an opioid antagonist and blocks the effect of opioid pain medications.
Since phentermine, topiramate, bupropion, and naltrexone are available as single agents, clinicians
may also use them “off label” alone and in various combinations for weight loss.
There are a host of other more invasive treatments including endoscopic surgical procedures and
devices placed into the stomach to promote early satiety. Though these may also be used for
individuals who have not achieved desired weight loss with lifestyle changes, patients and experts
felt that the limited time duration of weight loss and/or invasive nature of these procedures would
make them less comparable to medications that could be taken for longer periods.

©Institute for Clinical and Economic Review, 2022 Page 3
Evidence Report – Medications for Obesity Management Return to Table of Contents
Practical issues in using medications for weight loss are modest weight reduction, potential side
effects, long-term safety, durability of treatment effect, and concerns about insurance coverage.
Consequently, there is a need to understand the comparative benefits and costs of the newer
branded medications for individuals interested in weight loss after not achieving their goals with
initial lifestyle modification. Because semaglutide appears to promote greater weight loss than
other FDA-approved medications, there has been considerable interest among patients and
providers despite being administered as an injection and more costly.
Finally, a number of newer medications that promote weight loss are being investigated. An oral
version of semaglutide has been approved for the treatment of diabetes mellitus and is under
investigation for use in weight loss. Another medication, tirzepatide, is both a GLP-1 receptor
agonist and also a glucose-dependent insulinotropic polypeptide receptor agonist, and has been
approved for treatment of diabetes mellitus. Data on weight loss with tirzepatide have been
published,
12
and these results are discussed in Supplement A3.
Table 1.1. Interventions of Interest
Intervention
Mechanism of Action
Delivery Route
Prescribing Information
Semaglutide
GLP-1 receptor agonist
Subcutaneous
2.4 mg once weekly
Liraglutide
GLP-1 receptor agonist
Subcutaneous
3 mg once daily
Phentermine/Topiramate
Sympathomimetic amine/
GABA receptor modulation
Oral 7.5-15 mg/46-92 mg daily
Bupropion/Naltrexone
Opioid antagonist/NE and DA
inhibitor
Oral 32 mg/360 mg daily
CA: carbonic anhydrase, DA: dopamine, GABA: gamma-aminobutyric acid, GLP-1: glucagon-like peptide-1, mg:
milligram, NE: norepinephrine

©Institute for Clinical and Economic Review, 2022 Page 4
Evidence Report – Medications for Obesity Management Return to Table of Contents
2. Patient and Caregiver Perspectives
Discussions with individual patients and patient organizations identified important insights and
perspectives. Common themes emphasized included: the considerable physical and mental burden
on patients with obesity; the broad recognition that the social stigma associated with obesity can
begin at a young age and affect an individual throughout their life; the need for better treatment
options; the impact on all aspects of life including education, work and social/family relationships;
the importance of measuring treatment outcomes that are most meaningful to patients; and the
affordability of increasingly expensive treatments that may not be covered by health insurance.
Patients and clinicians emphasized that obesity is a serious, chronic disease with important health
consequences affecting both physical and mental well-being. Individuals with obesity are at
increased risk of chronic health conditions such as high blood pressure or cholesterol, diabetes
mellitus, heart disease, sleep apnea, arthritis, immobility, depression, and cancer. As a result,
obesity is associated with reduced disease-free life and increased risk of premature death.
28
Despite these risks, patients and advocates said that societal biases further the perception that
those living with obesity are not able to make the personal lifestyle choices to manage weight. This
simplistic focus on “blame the patient” overlooks considerable evidence that the causes of obesity
are complex and multifactorial. The resulting social stigma associated with obesity is widely felt by
individuals with obesity, begins at a young age, and affects individuals throughout their lives. This
stigma and bias can lead to anxiety, depression, and behaviors that make self-care harder, and may
impact willingness to engage with health care providers around weight loss and the consequences
of obesity.
We also heard that there are diverse perspectives about obesity that broadly reflect the many
individuals with obesity and the variety of underlying factors that contribute to obesity and its
management. Though many individuals with obesity are interested in weight loss, the cycle of
weight loss and gain, the many “fad” diets and treatments that offer unrealistic expectations, and
the cost of treatments that are often not covered by health insurance all impact perceptions about
weight loss. We heard some advocate more for efforts focused on managing the medical issues
associated with obesity, especially for those individuals who have suffered through failed
treatments, weight cycling, and the psychological harms associated with such prior experiences.
Even among those more interested in weight-neutral treatment efforts, there was recognition that
more can be done in the health care system to reduce the stigma of obesity and better support
individuals interested in weight loss treatment.
Patients and patient organizations identified that the impact of obesity is particularly high among
women and individuals from certain racial and ethnic groups. For example, the prevalence of
obesity is higher for Hispanic adults and highest among non-Hispanic Black women.
9,10
Moreover

©Institute for Clinical and Economic Review, 2022 Page 5
Evidence Report – Medications for Obesity Management Return to Table of Contents
disparities in access to health care and treatments for obesity may exacerbate the morbidity and
mortality associated with obesity across racial and ethnic groups. It was also highlighted that trials
of interventions for obesity need to ensure a diversity of individuals from different racial and ethnic
backgrounds.
Patients and clinicians highlighted that there is a need for new therapeutic options for individuals
with obesity who are interested in weight loss treatments, particularly for individuals who have not
responded to lifestyle treatments or who responded but then regained lost weight over time. They
emphasized that no one treatment is a panacea, and this reflects the various underlying
mechanisms that contribute to obesity as well as the benefits and harms associated with all
therapies. Given the wide variety of treatments available for those interested in weight loss
treatment, they supported focusing on medical therapies for those who have not responded to
lifestyle interventions and are interested in additional treatments. Though patients may also
consider invasive surgical and other device interventions while also considering the use of medical
therapies, patients felt that many individuals had treatment preferences that made direct
comparison of medical and non-medical therapies less important. This also reflected increased
interest in medications that provide substantial weight loss to an increasing percentage of users,
with weight reduction that is becoming comparable to results associated with some bariatric
procedures.
Patients and clinicians also reported that individuals with obesity commonly use medications
approved in combination products for weight loss but available as individual drugs in an off-label
manner. This reflected that they often saw this route as minimizing side effects when starting
treatment and being less costly for patients given the higher costs of approved combination
medications that are often not covered by insurers. The net effect is that many patients end up on
a combination of medications, but not always using the approved combination products. There was
also recognition that the addition of medications, such as the GLP-1 receptor agonists, represents a
step forward in the magnitude of weight loss achieved, but they do not work for everyone, and the
weight loss achieved is still less than that seen for bariatric surgery for many individuals. Finally, it is
acknowledged that most patients will require chronic use to maintain the weight loss achieved, not
unlike the need to use medications to manage diabetes mellitus, but there was concern about the
safety of long-term use and the willingness of individuals to remain on therapy for many years,
especially if it requires considerable out-of-pocket costs to the individual.

©Institute for Clinical and Economic Review, 2022 Page 6
Evidence Report – Medications for Obesity Management Return to Table of Contents
3. Comparative Clinical Effectiveness
3.1. Methods Overview
Procedures for the systematic literature review assessing the evidence on semaglutide, liraglutide,
phentermine/topiramate, and bupropion/naltrexone for the management of obesity are detailed in
Section D1
of the Supplement.
Scope of Review
We reviewed the clinical effectiveness of the medications plus lifestyle interventions compared to
placebo plus lifestyle interventions. For studies evaluating multiple doses or combinations of the
medications, we reviewed only the FDA-approved dose and/or combination for the obesity
indication. Lifestyle interventions were variably defined in the clinical trials as interventions ranging
from diet and exercise counseling to intensive behavioral therapy (IBT) and meal replacement
programs. We sought evidence on weight loss outcomes, including percentage weight loss from
baseline and proportion of participants achieving 5%, 10%, or 15% body weight loss as well as
patient-important outcomes, including functional status, health-related quality of life (HRQoL), and
weight regain. We also sought evidence on changes in glycated hemoglobin (A1C), systolic blood
pressure (SBP), low density lipoprotein (LDL), and waist circumference. The full scope of the review
is available in Section D1
of the Supplement.
Evidence Base
Semaglutide
Evidence informing our review of semaglutide for obesity management was derived from five of the
STEP trials. STEP 1, STEP 2, STEP 3, STEP 5, and STEP 8 were selected as studies of interest due to
their study design, relevant population, and length of follow-up.
29-33
Additional studies of
semaglutide are described in Section D2 and Tables D8, D13, and D19
in the Supplement.
STEP 1, STEP 2, and STEP 5 evaluated subcutaneous semaglutide 2.4 mg plus lifestyle intervention
versus placebo plus lifestyle intervention.
27,28,32
STEP 2 also evaluated subcutaneous semaglutide at
1.0 mg, but we only reviewed evidence for the subcutaneous semaglutide 2.4 mg as it is the
approved dose for obesity treatment (Table 3.3).
30
STEP 3 evaluated subcutaneous semaglutide 2.4
mg plus IBT versus placebo plus IBT (Table 3.1).
31
STEP 8 evaluated subcutaneous semaglutide 2.4
mg plus lifestyle intervention versus subcutaneous liraglutide 3.0 mg plus lifestyle intervention, and
compared both to placebo plus lifestyle intervention.
33
STEP 8 was open label due to dosing
differences between semaglutide and liraglutide, however, active treatment groups were double-
blinded to whether they were receiving the intervention or comparable placebo (Table 3.1).

©Institute for Clinical and Economic Review, 2022 Page 7
Evidence Report – Medications for Obesity Management Return to Table of Contents
Participants in STEP 1, 3, 5, and 8 included adults with BMI ≥30 kg/m
2
or ≥27 kg/m
2
with at least one
weight-related comorbid condition (Table 3.1).
29,31-33
History of type 1 or type 2 diabetes mellitus or
HbA1C equal to or above 6.5% were exclusion criteria for these trials. Participants in STEP 2
included adults with BMI of ≥27 kg/m² diagnosed with type 2 diabetes mellitus and excluded
individuals with renal disease (Table 3.3).
30
Participants in STEP 1, 3, 5, and 8 trials were of similar age and baseline weight and BMI.
29,31-33
Participants in STEP 2 who had diabetes mellitus were somewhat older, had lower BMI, and were
less likely to be female or White.
30
Baseline characteristics for the STEP trials are outlined in Tables
3.1 and 3.3. Outcomes were assessed at week 68 for all STEP trials except STEP 5, which evaluated
outcomes at weeks 52 and 104.
STEP 4, which was a withdrawal study, was not included in the base evidence review or network
meta-analysis (NMA) due to differences in study design and baseline weight loss during a run-in
dose escalation period.
33
However, we did review its unique data regarding weight regain. See
additional information regarding this trial in Section D2
of the Supplement.
Table 3.1. Overview of Key Trials of Semaglutide for the Management of Obesity
29,31,33-39
STEP 1
STEP 3
STEP 5
STEP 8
Study Arms
PBO
SEM
PBO
SEM
PBO
SEM
PBO
SEM
LIR
N
655
1,306
204
407
152
152
85
126
127
Lifestyle
Intervention
Monthly counseling,
reduced-calorie
diet, and increased
physical activity
Low calorie meal
replacement diet for
8 weeks and IBT visits
Monthly counseling,
reduced-calorie
diet, and increased
physical activity
Monthly counseling,
reduced-calorie diet,
and increased physical
activity
Mean Age,
Years
47 46 46 46 47 47 51 48 49
Female
Gender, %
76 73.1 88.2 77.4 74.3 80.9 77.6 81 76.4
Baseline
Weight, kg
105.2 105.4 103.7 106.9 106 108.8 102.5 103.7
Baseline
BMI, kg/m
2
38 37.8 37.8 38.1 38.5 38.8 37 37.2
Race, White,
%
76 74.5 77.5 75.4 93.4 92.8 70.6 74.6 74.8
Pre-Diabetes,
%
40.2 45.4 52.9 48.2 46.4 40 34.1 35.4
IBT: intensive behavioral therapy, kg: kilogram, LIR: liraglutide, m: meter, N: total number, NR: not reported, PBO:
placebo, SEM: semaglutide

©Institute for Clinical and Economic Review, 2022 Page 8
Evidence Report – Medications for Obesity Management Return to Table of Contents
Liraglutide
Evidence informing our review of liraglutide for obesity management was derived from six of the
SCALE Phase III randomized trials, which evaluated subcutaneous liraglutide 3.0 mg versus
placebo.
40-45
STEP 8, described previously, is included in the liraglutide evidence analysis as well.
33
Additional studies of liraglutide are described in Section D2 and in Tables D8, D13, and D19
of the
Supplement.
SCALE (Maintenance), SCALE (Sleep Apnea), SCALE (Obesity and Pre-Diabetes), and SCALE (Type 2
Diabetes) evaluated subcutaneous liraglutide 3.0 mg plus lifestyle intervention versus placebo plus
lifestyle intervention.
40-45
SCALE (IBT) and SCALE (Insulin) evaluated subcutaneous liraglutide 3.0 mg
plus IBT versus placebo plus IBT.
44,45
Participants in SCALE (IBT) included adults ages ≥18 with a BMI
≥30 kg/m
2
.
44
Participants in SCALE (Maintenance), SCALE (Sleep Apnea), and SCALE (Obesity and
Pre-Diabetes) included adults ages ≥18 with BMI ≥30kg/m
2
or ≥27kg/m
2
with untreated
dyslipidemia or hypertension.
40,41,43
SCALE
(Sleep Apnea) had additional inclusion criteria of
individuals with moderate to severe obstructive sleep apnea who were unable or unwilling to use
continuous positive airway pressure (CPAP).
41
Participants in SCALE (Type 2 Diabetes) included
adults ages ≥18 with overweight or obesity (BMI ≥27kg/m
2
) with a diagnosis of type 2 diabetes
mellitus treated with diet and exercise alone or one to three oral hypoglycemic medications.
42
Participants in SCALE (Insulin) included adults ages ≥18 with a BMI ≥27kg/m
2
, a
diagnosis of type 2
diabetes mellitus, and receiving stable treatment with any basal insulin and ≤2 oral hypoglycemic
medications.
45
All trials except SCALE (IBT) and SCALE (Insulin) excluded individuals with a history of
previous surgical treatment of obesity. Additionally, all studies excluded individuals with a recent
history of major depressive disorder or a lifetime suicide attempt. Any history of drug-induced
obesity or an endocrine disorder that could contribute to obesity (e.g., Cushing syndrome) was also
exclusion criteria across all trials. History of multiple endocrine neoplasia and familial medullary
thyroid carcinoma were also exclusionary due to the increased risk of medullary cancer of the
thyroid with GLP-1 receptor agonists.
46,47
Participants across all included trials were primarily
female, and of similar age and baseline weight and BMI, with some notable differences. SCALE
(Sleep Apnea) participants had higher baseline weight and were primarily male and participants in
SCALE (Type 2 Diabetes) and SCALE (Insulin) had higher baseline A1C and SBP.
41,42,45
Baseline
characteristics for the SCALE trials are outlined in Tables 3.2 and 3.3.
Outcomes were assessed at week 56 for all SCALE trials except SCALE (Sleep Apnea), which assessed
outcomes at week 32. SCALE (Type 2 Diabetes) additionally evaluated some relevant outcomes at
week 68.

©Institute for Clinical and Economic Review, 2022 Page 9
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 3.2. Overview of Key Trials of Liraglutide for the Management of Obesity
40,41,43,44,48-51
SCALE
Maintenance
SCALE
Sleep Apnea
SCALE
Obesity and
Pre-Diabetes
SCALE
IBT
Study Arms
PBO
LIR
PBO
LIR
PBO
LIR
PBO
LIR
N
210
212
179
180
1,244
2,487
140
142
Lifestyle
Intervention
Low-calorie run-in with
weekly counseling then
reduced-calorie diet,
and increased physical
activity
Monthly counseling,
reduced-calorie
diet, and increased
physical activity
Monthly counseling,
reduced-calorie diet,
and increased
physical activity
IBT, reduced-calorie
diet, and increased
physical activity
Mean Age,
Years
46.5 45.9 48.4 48.6 45 45.2 49 45.4
Female
Gender, %
78.6 84 27.9 28.3 78.1 78.7 82.9 83.8
Baseline
Weight, kg
98.7 100.4 118.7 116.5 106.2 106.2 106.7 108.5
Baseline
BMI, kg/m
2
35.2 36 39.4 38.9 38.3 38.3 38.7 39.3
Race, White,
%
88.1 80.2 75.4 72.2 85.3 84.7 82.1 78.9
Pre-Diabetes,
%
NR NR 62.6 63.9 60.9 61.4 NR NR
IBT: intensive behavioral therapy, kg: kilogram, LIR: liraglutide, m: meter, N: total number, NR: not reported, PBO:
placebo
Table 3.3. Overview of Key Trials of Semaglutide and Liraglutide for the Management of Obesity
with Diabetes
30,42,45,52
STEP 2
SCALE
Type 2 Diabetes
SCALE
Insulin
Study Arms
PBO
SEM
PBO
LIR
PBO
LIR
N
403
404
212
423
198
198
Lifestyle
Intervention
Monthly counseling,
reduced-calorie diet, and
increased physical activity
Monthly counseling,
reduced-calorie diet, and
increased physical activity
IBT, reduced-calorie diet, and
increased physical activity
Mean Age,
Years
55 55 54.7 55 57.6 55.9
Female
Gender, %
47.1 55.2 54.2 48 50 45.5
Baseline
Weight, kg
100.5 99.9 106.5 105.7 98.9 100.6
Baseline
BMI, kg/m
2
35.9 35.9 37.4 37.1 35.3 35.9
Race, White, %
60
58.7
82.5
83.5
90.9
87.9
IBT: intensive behavioral therapy, kg: kilogram, LIR: liraglutide, m: meter, N: total number, PBO: placebo, SEM:
semaglutide

©Institute for Clinical and Economic Review, 2022 Page 10
Evidence Report – Medications for Obesity Management Return to Table of Contents
Phentermine/Topiramate
Evidence informing our review of phentermine/topiramate for obesity management was derived
from three Phase III studies (EQUIP, EQUATE, and CONQUER). One additional Phase I/II study, OB-
204, is described in Section D2 and Tables D9, D16, and D20
of the Supplement.
EQUIP, EQUATE, and CONQUER were multi-center, Phase III randomized controlled trials that
evaluated phentermine 15 mg/topiramate 92 mg (high dose) plus lifestyle intervention versus
placebo plus lifestyle intervention (Table 3.4 and 3.5).
53-57
EQUIP also evaluated phentermine 3.75
mg/topiramate 23 mg and CONQUER evaluated the phentermine 7.5/topiramate 46 mg dose.
EQUATE had seven arms evaluating multiple doses of phentermine and topiramate monotherapy, in
addition to phentermine 7.5 mg/topiramate 46 mg. Evidence was reviewed only for phentermine
15 mg/topiramate 92 mg (high dose) and phentermine 7.5 mg/topiramate 46 mg doses (low dose),
and the NMA focused solely on the high dose.
The EQUIP, EQUATE, and CONQUER trials included adults ages 18-70, but each trial had varying BMI
requirements. EQUIP required that participants have a BMI of at least 35 kg/m
2
and EQUATE
included participants with a BMI of 30-45 kg/m
2
(Table 3.4).
53-57
The CONQUER trial required that
participants have a BMI of 27-45 kg/m
2
(with no lower BMI limit for patients who have diabetes
mellitus) and have at least two of the following comorbidities: SBP 140-160 mmHg (or 130-160
mmHg if diabetic), diastolic blood pressure 90-100 mmHg (or 85-100 mmHg if diabetic), or taking at
least two antihypertensive medications (Table 3.5).
53
The CONQUER trial additionally included both
adults with and without type 2 diabetes mellitus. For the purposes of our clinical review and NMA,
and due to the lack of data available in the subgroup of participants without diabetes mellitus, we
focused specifically on the diabetes mellitus subgroup in this trial because it comprised the majority
of participants (68%).
58
Having a serious medical condition, obesity of known endocrine origin, stage 2 hypertension,
previous surgery for obesity, or a weight change of >5 kg within three months were common
exclusion criteria for these trials. Patients in EQUIP and EQUATE were also excluded if they had
type 2 diabetes mellitus.
54,56
Additional exclusion criteria for CONQUER included fasting glucose
greater than 13 mmol/L, triglycerides greater than 4.52 mmol/L, use of antidiabetic medication
other than metformin, or a history of seizures or serious psychiatric illness.
53
EQUIP and EQUATE trials had similar baseline characteristics, except for BMI and weight.
54-57
The
BMI requirement was higher in EQUIP than in other trials, meaning that all participants in this trial
had severe obesity. As a result, the mean baseline BMI and body weight of participants was higher
in this trial compared to other trials in our review.
56
Compared to participants in EQUIP and
EQUATE, the diabetes mellitus subgroup of CONQUER had a higher mean age and fewer female
participants.
58
Baseline characteristics for these trials are reported in Tables 3.4 and 3.5.

©Institute for Clinical and Economic Review, 2022 Page 11
Evidence Report – Medications for Obesity Management Return to Table of Contents
Bupropion/Naltrexone
Evidence to inform our review of bupropion/naltrexone in patients with overweight or obesity was
derived from four Phase III randomized controlled trials, COR-I, COR-II, COR-BMOD, and COR
Diabetes. Two additional Phase III trials, CVOT Light and Ignite, are described in Section D2
and
Tables D9, D16, and D20 of the Supplement.
COR-I, COR-II, and COR Diabetes were multi-center, Phase III randomized controlled trials that
evaluated bupropion SR 360 mg/naltrexone SR 32 mg plus lifestyle intervention versus placebo plus
lifestyle intervention.
59-64
COR-I additionally evaluated a lower dose of bupropion SR 360
mg/naltrexone SR 16 mg, but we only reviewed the higher approved dose of the medication. COR-
BMOD was a multi-center, Phase III randomized controlled trial that evaluated bupropion SR 360
mg/naltrexone SR 32 mg plus IBT versus placebo plus IBT (Table 3.4 and 3.5).
65,66
COR-I, COR-II, and COR-BMOD included adults ages 18-65 years who had a BMI of 30-45 kg/m
2
, or a
BMI of 27-45 kg/m
2
with controlled hypertension and/or dyslipidemia (Table 3.4).
61,63,65
Inclusion
criteria for COR Diabetes included patients ages 18-70 years with a BMI of 27-45 kg/m
2
, who were
diagnosed with type 2 diabetes mellitus, had an HbA1C between 7-10%, fasting blood glucose <270
mg/dL, fasting triglycerides <400 mg/dL, SBP <145 mmHg, and diastolic blood pressure <95 mmHg
(Table 3.5).
59
Having type 1 diabetes mellitus, a serious medical condition, obesity of known endocrine origin,
surgery for obesity, a history of seizures, drug, or alcohol abuse, or using medications that affected
body weight were common exclusion criteria among the trials. Adults with overweight or obesity in
COR-I, COR-II, and COR-BMOD were additionally excluded if they had type 2 diabetes mellitus or a
weight change of >4 kg within three months.
61,63,65
In COR Diabetes, patients were also excluded if
they had diabetes mellitus secondary to pancreatitis or pancreatectomy, weight change >5 kg
within three months, or used diabetes medication or were not on a stable dose of oral antidiabetic
drugs.
59
Baseline characteristics for COR-I, COR-II, and COR-BMOD trials were similar,
61,63,65
except
participants in COR Diabetes were slightly older in age and less likely to be female.
59
Baseline data
for patients in these trials are reported in Tables 3.4 and 3.5.

©Institute for Clinical and Economic Review, 2022 Page 12
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 3.4. Overview of Key Trials of Phentermine/Topiramate and Bupropion/Naltrexone for the
Management of Obesity
54-57,61-66
EQUIP
EQUATE
COR-I
COR-II
COR-BMOD
Study Arms PBO
P/T
(high)
PBO
P/T
(low)
P/T
(high)
PBO B/N PBO B/N PBO B/N
N
514
512
109
107
108
581
583
495
1,001
202
591
Lifestyle
Intervention
LSM counseling,
reduced-calorie
diet, increased
physical activity
LSM counseling,
reduced-calorie diet,
increased physical
activity
LSM
counseling,
reduced-calorie
diet, increased
physical activity
LSM counseling,
reduced-calorie
diet, increased
physical activity
IBT, reduced-
calorie diet,
increased physical
activity
Mean Age,
Years
43 41.9 45 44.6 44.6 43.7 44.4 44.4 44.3 45.6 45.9
Female
Gender, %
82.7 82.8 78.9 79.4 78.7 85 85 84.8 84.6 91.6 89.3
Baseline
Weight, kg
115.8 115.2 100 102.2 99.3 99.5 99.7 99.2 100.3 101.9 100.2
Baseline
BMI, kg/m
2
42 41.9 36.2 36.6 35.9 36.2 36.1 36.1 36.2 37 36.3
Race,
White, %
79.7 80.4 76.1 74.8 81.5 75.7 75 83.6 83.4 73.7 68.5
Pre-
Diabetes, %
NR NR NR NR NR NR NR NR NR NR NR
B/N: bupropion/naltrexone, IBT: intensive behavioral therapy, kg: kilogram, LSM: lifestyle modification, m: meter,
N: total number, NR: not reported, PBO: placebo, P/T: phentermine/topiramate
Table 3.5. Overview of Key Trials of Phentermine/Topiramate and Bupropion/Naltrexone for the
Management of Obesity with Diabetes
53,58-60
CONQUER (Diabetes Subgroup)
COR Diabetes
Study Arms
PBO
P/T (low)
P/T (high)
PBO
B/N
N
157
67
164
159
265
Lifestyle Intervention
LSM counseling, reduced-calorie diet, increased
physical activity
LSM counseling, reduced-calorie
diet, increased physical activity
Mean Age, Years
52.6
52.5
52.1
53.8
53.9
Female Gender, %
71.3
65.6
62.1
52.8
54.3
Baseline
Weight, kg
99.3 97.2 103.2 105 106.3
Baseline
BMI, kg/m
2
36.2 35.3 37.1 36.3 36.7
Race, White, %
84.7
94
82.9
83
78.1
B/N: bupropion/naltrexone, kg: kilogram, LSM: lifestyle modification, m: meter, N: total number, PBO: placebo,
P/T: phentermine/topiramate

©Institute for Clinical and Economic Review, 2022 Page 13
Evidence Report – Medications for Obesity Management Return to Table of Contents
3.2. Results
The most common primary outcome reported was percentage weight loss from baseline to one
year after treatment initiation with dose escalation periods ranging from four to 16 weeks. Other
outcomes variably included categorical weight loss (participants achieving 5% or 10% weight loss),
and changes in metabolic and cardiovascular risk factors such as SBP, A1C, and LDL. As noted in the
prior section, trials differed in populations studied (such as participants with or without diabetes
mellitus or other conditions and baseline BMI) and intensity of lifestyle modification interventions
offered alongside active treatment or placebo (ranging from diet and exercise counseling to IBT).
To ensure comparability and generalizability of results, we present trials of participants with obesity
alone separately from trials of participants with obesity and diabetes mellitus.
Clinical trial participants for all interventions were also assessed for improvements in physical
function and mental HRQoL using a variety of instruments: Short Form 36v2 Health Survey (SF-
36v2), Impact of Weight on Quality of Life (IWQOL) Lite Clinical Trials Version, Patient Health
Questionnaire (PHQ-9), and Inventory of Depressive Symptomatology – Self Report (IDS-SR).
Changes in weight, SBP, A1C, and HRQoL as well as harms and discontinuation rates are
summarized below, and additional outcomes are available in Section D2
of the Supplement.
Clinical Benefits
For each medication, weight loss outcomes are summarized first followed by other outcomes (e.g.,
SBP and A1C). HRQoL outcomes are summarized for all drugs at the end of this section. For each
medication, results of trials conducted in patients with obesity are presented first, followed by trials
conducted in patients with obesity and diabetes mellitus.
Semaglutide versus Placebo
The efficacy of semaglutide compared with placebo for the management of obesity in patients
without diabetes mellitus was evaluated in three Phase III trials (STEP 1, 3, and 5).
29,31,38
In the STEP
1, 3, and 5 trials, participants in the subcutaneous semaglutide 2.4 mg arm consistently achieved
greater percent weight loss at one year (-15.6%, -16.5%, and -15.8%, respectively) versus placebo (-
2.8%, -5.8%, and -3.3%, respectively).
29,31,38
Similarly, for the co-primary outcomes of proportion of
participants who achieved at least 5% weight loss, at least 10% weight loss, and at least 15% weight
loss, a greater proportion of participants in the semaglutide arm achieved each categorical outcome
compared to participants in the placebo arm. Participants in the semaglutide arms of STEP 1, 3, and
5 trials also had greater improvements in SBP from baseline (-6.2 mmHg, -5.6 mmHg, and -6 mmHg,
respectively) compared to those in the placebo arms (-1.1 mmHg, -1.6 mmHg, and -1 mmHg,
respectively).
29,31
In the STEP 1, 3, and 5 trials, the absolute change in percentage A1C (change in
A1C) from baseline improved in the semaglutide arm (-0.45%, -0.51%, and -0.5%, respectively)
compared to the placebo arm (-0.15%, -0.27%, and -0.2%, respectively).
29,31,38
The absolute change

©Institute for Clinical and Economic Review, 2022 Page 14
Evidence Report – Medications for Obesity Management Return to Table of Contents
in percentage A1C for STEP 8 improved for the semaglutide arm (-0.2%) compared to an increase in
A1C for the placebo arm (0.1%).
31,33
See Table 3.6 for detailed results.
The efficacy of semaglutide for the management of obesity and type 2 diabetes mellitus was
evaluated through one Phase III trial (STEP 2).
30
Participants in the subcutaneous semaglutide 2.4
mg arm achieved greater percent weight loss at one year (-9.6%) versus placebo (-3.4%), but the
magnitude of weight loss appeared less than in the trials of participants without diabetes mellitus.
Similarly, for the co-primary outcomes of proportion of participants who achieved at least 5%
weight loss and at least 10% weight loss, a greater proportion of participants in the semaglutide
arm achieved each categorical outcome compared to participants in the placebo arm. Participants
in the semaglutide arm also had modest improvement in SBP (-3.6 mmHg) compared to those in the
placebo arm (-0.5 mmHg). Change in A1C from baseline was consistent across both the semaglutide
and placebo arms (-0.4% vs. -0.4%). See Table 3.8 for detailed results.
Physical functioning was assessed in the STEP 1, STEP 2, and STEP 3 trials using the SF-36v2 Physical
Functioning Score.
29-31
STEP 1 and 3 also assessed the mean change in baseline of the SF-36v2 PCS.
STEP 1 and 2 also assessed physical function utilizing the IWQOL-Lite-CT instrument.
29,30
Overall,
semaglutide resulted in greater improvement in the physical component across all HRQoL
instruments compared to placebo, indicating the intervention resulted in greater improvement in
health status for physical patient-reported outcomes. See Table D17
in the Supplement for detailed
results.
STEP 1, 2, and 3 trials all reported baseline SF-36v2 MCS scores, but only STEP 1 and 3 reported the
change from baseline to week 68. STEP 2 reported estimated treatment differences. In STEP 1,
participants in the semaglutide arm experienced improvement in SF-36 MCS scores (1.5) versus
placebo, which had a reduction in score (-2.1). Conversely, in STEP 3, participants in both treatment
arms experienced decreased SF-36 MCS, although there was a smaller decrease in the semaglutide
arm (-0.8) compared to placebo (-2.9). See Table D18 in the Supplement for detailed results.
Semaglutide versus Liraglutide
The efficacy of subcutaneous semaglutide versus subcutaneous liraglutide with a placebo
comparator for the management of obesity was evaluated in one Phase III trial (STEP 8).
33
Participants in the semaglutide 2.4 mg arm achieved greater weight loss at one year (-15.8%) versus
liraglutide 3.0 mg (-6.4%) and placebo (-1.9%). Similarly, for the co-primary outcomes of proportion
of participants who achieved at least 5% weight loss, at least 10% weight loss, and at least 15%
weight loss, a greater proportion of participants in the semaglutide arm achieved each categorical
outcome compared to participants in the liraglutide and placebo arms. Participants in the
semaglutide arm also had greater improvements in SBP from baseline (-5.7 mmHg) compared to
participants in the liraglutide arm (-2.9 mmHg), and participants in both the semaglutide and
liraglutide arms had greater improvement compared to those in the placebo arm, who had a

©Institute for Clinical and Economic Review, 2022 Page 15
Evidence Report – Medications for Obesity Management Return to Table of Contents
modest increase in SBP (3.2 mmHg). Minimal changes in A1C were seen in all arms of the trial. See
Table 3.6 for detailed results.
Table 3.6. Results of Key Trials of Semaglutide for the Management of Obesity
29,31,33-38,67
STEP 1
STEP 3
STEP 5
STEP 8
Study Arms
PBO
SEM
PBO
SEM
PBO
SEM
PBO
SEM
LIR
N
577
1,212
189
373
129
149
78
117
117
% Weight Loss from
Baseline to One Year,
Mean (SE)
-2.8
(0.3)†
-15.6
(0.3)†
-5.8
(0.4)†
-16.5
(0.5)†
-3.3
(0.6)†
-15.8
(0.8)†
-1.9
(1.1)†
-15.8
(0.9)†
-6.4
(0.9)†
Participants with at Least
5% Weight Loss, n (%)
182
(31.5)
1,047
(86.4)
90
(47.6)
323
(86.6)
38
(29.5)
132
(88.6)
23
(29.5)
102
(87.2)
68
(58.1)
Participants with at Least
10% Weight Loss, n (%)
69
(12)
838
(69.1)
51
(27)
281
(75.3)
17
(13.2)
102
(68.5)
12
(15.4)
83
(70.9)
30
(25.6)
Change in SBP from
Baseline, mmHg, Mean
(SE)
-1.1
(0.5)†
-6.2
(0.4)†
-1.6*
(1.1)
-5.6*
(0.7)
-1*
(1.2)‡
-7*
(1.1)†
3.2*
(1.5)†
-5.7*
(1.2)†
-2.9*
(1.2)†
Change in %HbA1C from
Baseline, Mean (SE)
-0.15*
(0.01)†
-0.45*
(0.01)†
-0.27*
(0.01)†
-0.51*
(0.02)†
-0.2*
(0.02)†
-0.5*
(0.03)†
0.1*
(0.02)†
-0.2*
(0.03)†
-0.1*
(0.03)†
HbA1C: glycated hemoglobin, LIR: liraglutide, mmHg: millimeters of mercury, n: number, N: total number, PBO:
placebo, SBP: systolic blood pressure, SE: standard error, SEM: semaglutide
*The number of patients for this outcome may differ from the primary analysis population.
†SE manually derived from standard deviation or 95% CIs.
Liraglutide versus Placebo
The efficacy of liraglutide compared with placebo for the management of obesity was evaluated in
four Phase III trials in the SCALE clinical trial program (Maintenance, Sleep Apnea, Obesity and Pre-
Diabetes, IBT).
40,41,43,44
In the Maintenance, Obesity and Pre-Diabetes, and IBT trials, participants in
the subcutaneous liraglutide 3.0 mg arm consistently achieved greater percent weight loss at one
year (-6.2%, -8%, and -7.4%, respectively) versus placebo (-0.2%, -2.6%, and -4%, respectively).
40,43,44
Similarly, for the co-primary outcomes of proportion of participants who achieved at least 5%
weight loss and at least 10% weight loss, a greater proportion of participants in the liraglutide arm
achieved each categorical outcome compared to participants in the placebo arm. Changes in SBP
varied across trials with liraglutide demonstrating modest improvements relative to placebo, except
in the Maintenance trial in which participants in both the liraglutide and placebo arms experienced
an increase in SBP from baseline (0.2 mmHg and 2.8 mmHg, respectively).
40
Across all four SCALE
trials, greater improvements in change in A1C were consistently demonstrated in the liraglutide
arm compared to the placebo arm, although the results varied between studies.
40,41,43,44
See Table
3.7 for detailed results.
The efficacy of subcutaneous liraglutide compared with placebo for the management of obesity
with diabetes mellitus was evaluated in two Phase III trials in the SCALE clinical trial program (Type
2 Diabetes, Insulin).
42,45
In both the SCALE (Type 2 Diabetes) and SCALE (Insulin) trials, participants

©Institute for Clinical and Economic Review, 2022 Page 16
Evidence Report – Medications for Obesity Management Return to Table of Contents
in the liraglutide 3.0 mg arm had greater percent weight loss at one year (-5.9% and -5.8%,
respectively) compared to placebo (-2% and -1.5%, respectively). Similarly, liraglutide
demonstrated a greater proportion of participants who achieved at least 5% or 10% weight loss
compared to placebo. Liraglutide also demonstrated greater improvements in SBP compared to
placebo. Across both trials, improvements in A1C were greater in the liraglutide arms (-1.3% and -
1.1%, respectively) compared to the placebo arms (-0.3% and -0.6%, respectively). See Table 3.8 for
detailed results.
The SCALE (Sleep Apnea, Obesity and Pre-Diabetes, IBT, and Insulin) trials assessed physical patient-
reported outcomes utilizing the SF-36v2 PCS instrument.
41,43-45
The IWQOL-Lite-CT instrument
assessed physical function score in the SCALE (Type 2 Diabetes, Obesity and Pre-Diabetes, IBT, and
Insulin) studies.
42-45
Overall, liraglutide resulted in greater improvement in the physical component
across all HRQoL instruments compared to placebo, indicating the intervention resulted in greater
improvement in health status for physical patient-reported outcomes. The one exception was
SCALE (IBT), which reported slightly less improvement in SF-36v2 PCS scores for liraglutide (3.4)
compared to placebo (3.8). See Table D17
in the Supplement for detailed results.
Four studies for liraglutide, SCALE (Sleep Apnea, Obesity and Pre-Diabetes, IBT, and Insulin) trials
also evaluated the mental component utilizing the SF-36v2 MCS instrument with minimal
improvements compared to baseline in the liraglutide arm for the SCALE (Sleep Apnea and Obesity
and Pre-Diabetes) trials (1.4 and 0.2, respectively), less improvement in the SCALE (Sleep Apnea)
placebo arm (0.9), and a decrease in health quality in the SCALE (Obesity and Pre-Diabetes) placebo
arm (-0.9).
41,43
The SCALE (IBT and Insulin) trials reported a decrease in SF-36v2 scores across both
the liraglutide and placebo arms of the trial, indicating a decreased mental health status. See
Table
D18 in the Supplement for detailed results.

©Institute for Clinical and Economic Review, 2022 Page 17
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 3.7. Results of Key Trials of Liraglutide for the Management of Obesity
40,41,43,44,48-51,67
SCALE
Maintenance
SCALE
Sleep Apnea‡
SCALE
Obesity and
Pre-Diabetes
SCALE
IBT
Study Arms
PBO
LIR
PBO
LIR
PBO
LIR
PBO
LIR
N
188
194
178
175
1,220
2,432
130
141
% Weight Loss from
Baseline to One Year,
Mean (SE)
-0.2†
(0.5)*
-6.2†
(0.5)*
N/A N/A
-2.6
(0.2)*
-8
(0.1)*
-4
(0.6)*
-7.4
(0.7)*
Participants with 5%
Weight Loss, n (%)
41
(21.8)
98
(50.5)
33
(18.5)
81
(46.3)
331
(27.1)
1,537
(63.2)
50
(38.8)
87
(61.5)
Participants with 10%
Weight Loss, n (%)
12
(6.3)
51
(26.1)
3
(1.7)
41
(23.4)
129
(10.6)
805
(33.1)
26
(19.8)
43
(30.5)
Change in SBP from
Baseline, mmHg,
Mean (SE)
2.8†
(0.7)*
0.2†
(0.8)*
0† (1)
-3.4†
(0.9)
-1.5†
(0.4)*
-4.2†
(0.2)*
-0.6† (NR)
-2.8†
(NR)
Change in %HbA1C
from Baseline, Mean
(SE)
0.1†
(0.03)*
-0.1†
(0.03)*
-0.2† (0) -0.4† (0)
-0.06†
(0.01)*
-0.3†
(0.01)*
-0.06†
(0.02)*
-0.16†
(0.03)*
A1C: glycated hemoglobin, LIR: liraglutide, mmHg: millimeters of mercury, n: number, N: total number, N/A: not
applicable, NR: not reported, PBO: placebo, SBP: systolic blood pressure, SE: standard error
*SE manually derived from standard deviation or 95% CIs.
†The number of patients for this outcome may differ from the primary analysis population.
‡Timepoint is at week 32 for all outcomes.
Table 3.8. Results of Key Trials of Semaglutide and Liraglutide for the Management of Obesity
with Diabetes Mellitus
30,42,45,52,67
STEP 2
SCALE
Type 2 Diabetes
SCALE
Insulin
Study Arms
PBO
SEM
PBO
LIR
PBO
LIR
N
376
388
211
412
193
191
% Weight Loss from
Baseline to One Year,
Mean (SE)
-3.4 (0.4) -9.6 (0.4) -2 (0.3)* -5.9 (0.3)* -1.5 (0.4) -5.8 (0.4)
Participants with 5%
Weight Loss, n (%)
107 (28.5) 267 (68.8) 45 (21.4) 224 (54.3) 46 (24) 100 (51.8)
Participants with 10%
Weight Loss, n (%)
31 (8.2) 177 (45.6) 14 (6.7) 104 (25.2) 13 (6.6) 44 (22.8)
Change in SBP from
Baseline, mmHg,
Mean (SE)
-0.5† (0.8) -3.9† (0.7) -0.4† (0.9)* -2.8† (0.7)* -1.6† (0.9) -5.6† (0.9)
Change in %HbA1C
from Baseline, Mean
(SE)
-0.4† (0.1) -0.4† (0.1)
-0.3†
(0.06)*
-1.3† (0.04)* -0.6† (NR) -1.1† (NR)
A1C: glycated hemoglobin LIR: liraglutide, mmHg: millimeters of mercury, n: number, N: total number, NR: not
reported, PBO: placebo, SBP: systolic blood pressure, SE: standard error, SEM: semaglutide
*SE manually derived from standard deviation or 95% CIs.
†The number of patients for this outcome may differ from the primary analysis population.

©Institute for Clinical and Economic Review, 2022 Page 18
Evidence Report – Medications for Obesity Management Return to Table of Contents
Phentermine/Topiramate versus Placebo
In the EQUIP trial, participants in the phentermine 15 mg/topiramate 92 mg arm achieved greater
weight loss at one year (-10.9%) than participants in the placebo arm (-1.6%).
56,57
For the co-
primary outcome of proportion of participants who lost at least 5% of their weight, more
participants in the phentermine/topiramate arm achieved this outcome compared to participants in
the placebo group. Similarly, more participants in the high-dose treatment arm achieved 10%
weight loss compared to the placebo arm (Table 3.9).
One-year outcomes were not available in the EQUATE trial, whose timepoints went out to only 28
weeks.
Participants in the diabetes mellitus subgroup of the CONQUER trial receiving phentermine 15 mg/
topiramate 92 mg treatment (high dose) and phentermine 7.5 mg/topiramate 46 mg (low dose)
achieved a greater weight improvement at one year (-8.8% and -6.8%, respectively) than
participants in the placebo arm (-1.9%).
53,58
Categorical weight loss of at least 5% and 10% were not
assessed in this diabetes mellitus subgroup population. See Table 3.10 for detailed results.
In terms of secondary outcomes, in the EQUIP trial, SBP decreased by 2.9 mmHg in the high-dose
phentermine/topiramate arm and increased by 0.9 mmHg in the placebo arm (Table 3.9).
56
In the
CONQUER diabetes mellitus subgroup, patients in the high-dose phentermine/topiramate arm and
low-dose phentermine/topiramate arm experienced HbA1C decreases of 0.4% compared to the
placebo decreases of 0.1%.
53
Similarly, in patients with diabetes mellitus in CONQUER, SBP
decreased by 4.2 mmHg in the phentermine 15 mg/topiramate 92 mg group, by 2.9 mmHg in the
phentermine 7.5 mg/topiramate 46 mg group, and by 2.1 mmHg in the placebo group (Table
3.10).
58
Physical function outcomes were not assessed. Depression was assessed in the EQUATE and EQUIP
trials using the PHQ-9 instrument. For both trials, a greater improvement in this measure was
observed in the high-dose phentermine/topiramate arms, compared to the placebo arms. In
EQUATE, participants in the high-dose and low-dose phentermine/topiramate arms improved by 1.1
and 1.3 points, respectively, while participants in placebo improved by 0.5 points.
54,55
Depression
scores in the EQUIP trial improved more from baseline in the high-dose phentermine/topiramate
group (1.5), compared to the placebo group (1.3).
56,57
PHQ-9 was not assessed in the diabetes
mellitus subgroup of the CONQUER trial. See Table D18
in the Supplement for detailed results.

©Institute for Clinical and Economic Review, 2022 Page 19
Evidence Report – Medications for Obesity Management Return to Table of Contents
Bupropion/Naltrexone versus Placebo
In the COR-I, COR-II, and COR-BMOD trials of adults with obesity, participants in the bupropion 360
mg/naltrexone 32 mg (high dose) arm achieved greater weight loss at one year (-6.1%, -6.4%, and
-9.3%, respectively), than participants in the placebo arm (-1.3%, -1.2%, and -5.1%, respectively).
61-
63,65,66
For the co-primary outcome of participants who lost at least 5% of their weight, a greater
proportion of participants in the intervention arm achieved this outcome compared to placebo. A
similar pattern was observed for the secondary outcome of proportion of participants who achieved
10% weight loss between the arms. See Table 3.9 for detailed results.
Participants in the bupropion 360 mg/naltrexone 32 mg arm in the COR Diabetes trial achieved
greater percent weight loss at one year (-5%) than participants in the placebo arm (-1.8%).
59,60
For
the co-primary outcome of proportion of participants who lost at least 5% of their weight, more
participants in the bupropion/naltrexone arm achieved this outcome compared to participants in
the placebo group. Additionally, more participants in the treatment arm achieved 10% weight loss
than in the placebo arm (Table 3.10).
In COR-I, SBP decreased by 0.1 mmHg in participants receiving the intervention and by 1.9 mmHg in
participants receiving placebo (Table 3.9).
57,58,61,62
A similar pattern was observed in the COR-
BMOD trial, where SBP decreased by 1.3 mmHg in the bupropion/naltrexone group versus 3.9
mmHg in the placebo group.
65
In the COR-II trial, SBP increased by 0.6 mmHg in the treatment
group and decreased by 0.5 mmHg in the placebo group (p=0.039).
63
None of these trials assessed
HbA1C levels.
In the COR Diabetes trial, change from baseline in HbA1C was -0.63% in the treatment group, and
-0.14% in the placebo arm.
59
Participants receiving the treatment experienced no change in SBP,
while participants receiving placebo experienced a mean decrease in SBP of 1.1 mmHg. See Table
3.10 for detailed results.
HRQoL was assessed using the IWQOL-Lite, an obesity-specific instrument and the IDS-SR, which
assesses depressive symptoms. In COR-I, COR-II, and COR-BMOD, patients in the
bupropion/naltrexone group showed a greater improvement in the IWQOL-LITE physical function
and total scores than patients in the placebo group.
61-63,65,66
However, changes in depression scores
were not consistent across trials. In COR-I and COR-II, patients in the placebo arm reported a
greater improvement in their depressive symptoms (-0.7 and -0.5, respectively) compared to the
high-dose bupropion/naltrexone arm (-0.3) (lower is better).
61-63
In COR-BMOD, patients in the
treatment arm reported a 0.1 increase from baseline in IDS-SR score, meaning their depressive
symptoms worsened, while patients in placebo reported no change.
65,66
In the COR Diabetes trial,
patients in the bupropion/naltrexone treatment arm reported no change in depression score, while
patients in the placebo arm reported that their mean score improved by 1.6.
59,60
See Tables D17
and D18 in the Supplement for detailed results.

©Institute for Clinical and Economic Review, 2022 Page 20
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 3.9. Results of Key Trials of Phentermine/Topiramate and Bupropion/Naltrexone for the
Management of Obesity
56,57,61-66
EQUIP
COR-I
COR-II
COR BMOD
Study Arms PBO
P/T
(high)
PBO B/N PBO B/N PBO B/N
N
498
498
511
471
456
702
193
482
% Weight Loss from
Baseline to One Year,
Mean (SE)
-1.6
(0.4)
-10.9
(0.4)
-1.3
(0.3)
-6.1
(0.3)
-1.2
(0.3)
-6.4
(0.3)
-5.1
(0.6)
-9.3
(0.4)
Participants with 5%
Weight Loss, n (%)
86
(17.3)
332
(66.7)
84 (16) 226 (48)
80
(17.1)
354
(50.5)
82
(42.5)
320
(66.4)
Participants with 10%
Weight Loss, n (%)
37 (7.4)
235
(47.2)
38 (7) 116 (25) 26 (5.7)
199
(28.3)
39
(20.2)
200
(41.5)
Change in SBP from
Baseline, mmHg, Mean
(SE)
0.9
(0.6)*
-2.9
(0.6)*
-1.9
(0.4)
-0.1
(0.4)
-0.5
(0.4)
0.6
(0.3)
-3.9
(0.7)
-1.3
(0.5)
Change in %HbA1C from
Baseline, Mean (SE)
NR NR NR NR NR NR NR NR
A1C: glycated hemoglobin, B/N: bupropion/naltrexone, mmHg: millimeters of mercury, n: number, N: total
number, NR: not reported, PBO: placebo, P/T: phentermine/topiramate, SBP: systolic blood pressure, SE: standard
error
*SE manually derived from standard deviation or 95% CIs.
Table 3.10. Results of Key Trials of Phentermine/Topiramate and Bupropion/Naltrexone for the
Management of Obesity with Diabetes Mellitus
53,58-60
CONQUER (Diabetes Subgroup)
COR Diabetes
Study Arms
PBO
P/T (low)
P/T (high)
PBO
B/N
N
157
67
164
159
265
% Weight Loss from
Baseline to One Year, Mean
(SE)
-1.9 (0.6)* -6.8 (0.9)* -8.8 (0.6)* -1.8 (0.4) -5 (0.3)
Participants with 5%
Weight Loss, n (%)
NR NR NR 30 (18.9) 118 (44.5)
Participants with 10%
Weight Loss, n (%)
NR NR NR 9 (5.7) 49 (18.5)
Change in SBP from
Baseline, mmHg, Mean (SE)
-2.1 (1.1) -2.9 (1.6) -4.2† (1) -1.1 (0.9) 0 (0.7)
Change in %HbA1C from
Baseline, Mean (SE)
-0.1†
(0.05)*
-0.4† (1.5)* -0.4† (0.6)* -0.14† (0.09) -0.63† (0.07)
A1C: glycated hemoglobin, BN: bupropion/naltrexone, mmHg: millimeters of mercury, n: number, N: total number,
NR: not reported, PBO: placebo, PT: phentermine/topiramate, SBP: systolic blood pressure, SE: standard error
*SE manually derived from standard deviation or 95% CIs.
†The number of patients for this outcome may differ from the primary analysis population.

©Institute for Clinical and Economic Review, 2022 Page 21
Evidence Report – Medications for Obesity Management Return to Table of Contents
NMA Results of Percentage Weight Loss from Baseline at One Year
We conducted NMAs of trials including participants with obesity alone separately from trials of
participants with obesity and diabetes mellitus and excluded trials that included IBT as an adjunct to
medication. The primary outcome NMAs are reported below, and additional outcomes are
available in Supplement D1
.
Participants with Obesity Alone
For the trials of the medications conducted in participants with obesity without diabetes mellitus
that included standard diet and exercise counseling and reported percentage weight loss at one
year, we present the results of the baseline risk-adjusted random effects model, given its better fit
for the model compared to the unadjusted model in Table 3.11. All medications, in combination
with diet and exercise counseling, showed statistically significantly greater mean weight loss than
placebo with diet and exercise counseling at one year. Compared to placebo, the interventions
demonstrated 4.6-13.7% mean greater weight loss. Semaglutide demonstrated the greatest
percentage weight loss at one year and was superior to all other medications in our review for this
outcome. Phentermine/topiramate (high dose) demonstrated greater weight loss than liraglutide
and bupropion/naltrexone, however, liraglutide was not statistically more effective in
demonstrating weight loss than bupropion/naltrexone (Table 3.11).
Table 3.11. NMA Results of Medications for the Management of Obesity, Mean Percentage
Weight Loss from Baseline at One Year (95% CI)
Semaglutide
-4.6 (-2.4 to -7.2)
Phentermine/
Topiramate*
-8.7 (-7.3 to -10.4) -4.1 (-1.9 to -6.3) Liraglutide
-9.1 (-7.2 to -11.5) -4.5 (-2.2 to -6.9) -0.4 (-2.3 to +1.3)
Bupropion/
Naltrexone
-13.7 (-12.6 to -15.1) -9.1 (-7.1 to -11) -5.0 (-3.9 to -6.1) -4.6 (-3.0 to -6.0) Placebo
Legend: Each cell represents estimated absolute differences in percentage weight loss and 95% credible interval
for the combined direct and indirect comparisons between two medications or one medication and placebo.
Estimates in bold indicate the 95% credible interval does not contain 1.
*High dose.

©Institute for Clinical and Economic Review, 2022 Page 22
Evidence Report – Medications for Obesity Management Return to Table of Contents
Participants with Obesity and Diabetes Mellitus
For the trials of the medications conducted in participants with obesity and diabetes mellitus (using
the approved obesity indication dose) that reported percentage weight loss at one year, we present
the results of the baseline risk-adjusted random effects model, given its better fit for the model
compared to the unadjusted model in Table 3.12. All medications, in combination with diet and
exercise counseling, showed statistically significantly greater mean weight loss than placebo with
diet and exercise counseling at one year among participants with obesity with diabetes mellitus,
although the magnitude of the weight loss was somewhat lower than in trials of participants with
obesity alone, especially for semaglutide. Compared to placebo, the medications demonstrated
2.9-7.6% mean greater weight loss at one year. Semaglutide demonstrated a greater percentage
weight loss among the medications, however, these differences were not statistically significant.
Phentermine/topiramate (high dose) demonstrated greater weight loss than liraglutide and
bupropion/naltrexone, however, the results were only statistically significant compared to
bupropion/naltrexone. Liraglutide was not statistically more effective in demonstrating weight loss
than bupropion/naltrexone (Table 3.12).
Table 3.12. NMA Results of Medications for the Management of Obesity with Diabetes Mellitus,
Mean Percentage Weight Loss from Baseline at One Year (95% CI)
Semaglutide
-0.9 (-6.3 to +6.2)
Phentermine/
Topiramate*
-3.9 (-9.3 to +3.7) -2.9 (-0.05 to -5.8) Liraglutide
-4.7 (-10.3 to +2.8) -3.8 (-0.4 to -7.1) -0.9 (-3.8 to +2.1)
Bupropion/
Naltrexone
-7.6 (-1.7 to -11.9) -6.7 (-4.2 to -9.2) -3.7 (-1.7 to -6) -2.9 (-0.4 to -5.6) Placebo
Legend: Each box represents estimated absolute differences in percentage weight loss and 95% credible interval
for the combined direct and indirect comparisons between two medications or one medication and placebo.
Estimates in bold indicate the 95% credible interval does not contain 1.
*High dose.
NMA Results of Change in SBP from Baseline at One Year
Participants with Obesity Alone
For the trials of the medications conducted in participants with obesity without diabetes mellitus
that included standard diet and exercise counseling and reported change in SBP at one year, we
present the results of the baseline risk-adjusted random effects model, given its better fit for the
model compared to the unadjusted model in Table 3.13. All medications, in combination with diet
and exercise counseling, showed statistically significantly greater improvements in SBP than
placebo with diet and exercise counseling at one year except bupropion/naltrexone, which was

©Institute for Clinical and Economic Review, 2022 Page 23
Evidence Report – Medications for Obesity Management Return to Table of Contents
comparable to placebo. Compared to placebo, the interventions demonstrated 3.8-7.1 mmHg
improvements in SBP. Semaglutide demonstrated the greatest improvement in SBP at one year and
was superior to all other medications in our review except for phentermine/topiramate (high dose)
for this outcome. Phentermine/topiramate (high dose) and liraglutide both demonstrated greater
improvements in SBP than bupropion/naltrexone, however, the interventions were statistically
equivalent (Table 3.13).
Table 3.13. NMA Results of Medications for the Management of Obesity, Mean Change in SBP
from Baseline at One Year (95% CI)
Semaglutide
-2.9 (-6.2 to 0.4)
Phentermine/
Topiramate*
-3.3 (-5.3 to -1.2) -0.4 (-3.6 to 2.9) Liraglutide
-6.3 (-7.9 to -4.7) -3.4 (-6.3 to -0.6) -3.1 (-4.7 to -1.4) Placebo
-7.1 (-9.8 to -4.4) -4.2 (-7.9 to -0.6) -3.9 (-6.8 to -1.0) -0.8 (-3.0 to 1.3)
Bupropion/
Naltrexone
Legend: Each box represents estimated absolute differences in SBP and 95% credible interval for the combined
direct and indirect comparisons between two medications or one medication and placebo. Estimates in bold
indicate the 95% credible interval does not contain 1.
*High dose.
Participants with Obesity and Diabetes Mellitus
For the trials of the medications conducted in participants with obesity and diabetes mellitus and
reported change in SBP at one year, we present the results of the baseline risk-adjusted random
effects model, given its better fit for the model compared to the unadjusted model in Table 3.14.
Semaglutide and liraglutide, in combination with diet and exercise counseling, showed statistically
significantly greater improvements in SBP than placebo with diet and exercise counseling at one
year, while phentermine/topiramate (high dose) and bupropion/naltrexone did not. Compared to
placebo, semaglutide and liraglutide demonstrated 4.3 mmHg and 3.4 mmHg improvements in SBP,
respectively (Table 3.14).

©Institute for Clinical and Economic Review, 2022 Page 24
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 3.14. NMA Results of Medications for the Management of Obesity and Diabetes Mellitus,
Mean Change in SBP from Baseline at One Year (95% CI)
Semaglutide
-0.9 (-4.2 to 2.5) Liraglutide
-3.5 (-8.9 to 2.1) -2.7 (-6.8 to -1.6)
Phentermine/
Topiramate*
-4.3 (-1.2 to -7.2) -3.4 (-1.6 to -5.2) -0.7 (-4.4 to 2.8)
Placebo
-5.3 (-1.4 to -9.2) -4.4 (-1.3 to -7.6) -1.8 (-6.3 to 2.6) -1.1 (-4.6 to 1.5)
Bupropion/
Naltrexone
Legend: Each box represents estimated absolute differences in SBP and 95% credible interval for the combined
direct and indirect comparisons between two medications or one medication and placebo. Estimates in bold
indicate the 95% credible interval does not contain 1.
*High dose.
Harms
Adverse events reported in the trials are detailed below by medication. It is worth noting that three
of the medications carry black box warnings and the fourth has a Risk Evaluation and Mitigation
Strategies in place. The GLP-1 medications, semaglutide and liraglutide, carry a black box warning
for thyroid carcinoma and bupropion/naltrexone carries a warning for suicidality.
Phentermine/topiramate has a Risk Evaluation and Mitigation Strategy in place for a risk of birth
defects. These outcomes were not observed in any of the trials but relate to real-world data and
should be taken into consideration when prescribing.
Semaglutide
The most frequent adverse events in the STEP trials for semaglutide were gastrointestinal-related
symptoms, including nausea, constipation, and diarrhea.
29-38
Beyond gastrointestinal events,
semaglutide appeared relatively well-tolerated. Rates of adverse events and serious adverse events
were higher in the semaglutide arm compared to placebo, except STEP 5, which had a higher rate of
serious adverse events in the placebo arm (11.8%) versus the semaglutide arm (7.9%) (Table 3.15).
The higher rate of serious adverse events in the placebo arm of STEP 5 seems to be a chance event
associated with events that are not expected to be associated with the intervention within the
placebo arm, including COVID-19 infections, foot deformity, jaw and rib fractures, and several
occurrences of cancer.
37,38
Across all trials, there were higher rates of discontinuation due to adverse events in the
semaglutide arms compared to placebo, and discontinuation was most often attributed to
gastrointestinal events. In STEP 8, participants in the liraglutide arm were more likely to
discontinue due to adverse events (12.6%) compared to both the semaglutide and placebo arms

©Institute for Clinical and Economic Review, 2022 Page 25
Evidence Report – Medications for Obesity Management Return to Table of Contents
(3.2% and 3.5%, respectively) (safety analysis set).
33
STEP 2, which evaluated participants with
obesity and diabetes mellitus, did not exhibit any significant differences in harms compared to
other trials in the STEP clinical trial program, which evaluated participants with obesity without
diabetes mellitus.
30
See Table 3.15 for detailed harms results.
There were several areas of focus for safety in the STEP clinical trial program due to therapeutic
experience with GLP-1 receptor agonists and regulatory feedback and requirements. These
included gastrointestinal disorders, gallbladder-related disorders, cardiovascular disorders, and
psychiatric disorders. As expected, there were higher rates of gastrointestinal disorders in
semaglutide arms as compared to placebo across all trials.
68
In STEP 1, 3, and 5 trials, gallbladder-
related disorders were more frequent in the semaglutide arms compared to placebo, and
cardiovascular disorders were observed more in the placebo arm than in semaglutide
29,31,38
In STEP
2 and STEP 8, rates of gallbladder-related disorders were higher in placebo arm than in semaglutide,
and rates of cardiovascular disorders were higher in the semaglutide arms than placebo
30,33
.
Psychiatric disorder event rates were higher in semaglutide arms versus placebo arms in the STEP 2,
STEP 3, and STEP 5 trials. In the STEP 8 trial, there were higher rates of psychiatric disorder events
in the liraglutide arm (15%) compared to the semaglutide (5.6%) and placebo arms (10.6%).
33
See
Supplement Table D33
for detailed safety focus area results.
Table 3.15. Harms in Key Trials of Semaglutide for the Management of Obesity or Obesity with
Diabetes Mellitus
29-38
STEP 1
STEP 2*
STEP 3
STEP 5
STEP 8
Study Arms
PBO
SEM
PBO
SEM
PBO
SEM
PBO
SEM
PBO
SEM
LIR
N
655
1,306
402
403
204
407
152
152
85
126
127
Any AE, n (%)
566
(86.4)
1,171
(89.7)
309
(76.9)
353
(87.6)
196
(96.1)
390
(95.8)
136
(89.5)
146
(96.1)
81
(95.3)
120
(95.2)
122
(96.1)
SAE, n (%)
42
(6.4)
128
(9.8)
37
(9.2)
40
(9.9)
6
(2.9)
37
(9.1)
18
(11.8)
12
(7.9)
6
(7.1)
10
(7.9)
14 (11)
AEs Leading to
Discontinuation, n
(%)
20
(3.1)
92
(7)
14
(3.5)
25
(6.2)
6
(2.9)
24
(5.9)
7
(4.6)
9
(5.9)
3
(3.5)
4
(3.2)
16
(12.6)
GI Disorders
Leading to
Discontinuation, n
(%)
5
(0.8)
59
(4.5)
4 (1)
17
(4.2)
0 (0)
14
(3.4)
NR NR
1
(1.2)
1
(0.8)
8 (6.3)
Nausea, n (%)
114
(17.4)
577
(44.2)
37
(9.2)
136
(33.7)
45
(22.1)
237
(58.2)
NR NR
19
(22.4)
77
(61.1)
75
(59.1)
Constipation, n (%)
62
(9.5)
306
(23.4)
22
(5.5)
70
(17.4)
50
(24.5)
150
(36.9)
NR NR
20
(23.5)
49
(38.9)
40
(31.5)
Diarrhea, n (%)
104
(15.9)
412
(31.5)
48
(11.9)
86
(21.3)
45
(22.1)
147
(36.1)
NR NR
22
(25.9)
35
(27.8)
23
(18.1)
AE: adverse event, GI: gastrointestinal, LIR: liraglutide, n: number, N: total number, NR: not reported, PBO:
placebo, SAE: serious adverse event, SEM: semaglutide
*Included participants with obesity and diabetes mellitus.

©Institute for Clinical and Economic Review, 2022 Page 26
Evidence Report – Medications for Obesity Management Return to Table of Contents
Liraglutide
Like semaglutide, the most frequent adverse events in the SCALE trials for liraglutide compared with
placebo were gastrointestinal-related symptoms, including nausea, constipation, and diarrhea.
40-
45,48,50-52
The frequency of any adverse events was similar between liraglutide and placebo across all
trials, with the exception of the SCALE (Obesity and Pre-Diabetes) trial, in which participants in the
liraglutide arm experienced a higher rate of any adverse events (80.3%), regardless of causality,
compared to participants in the placebo arm (63.3%).
43
Rates of discontinuation due to adverse
events were higher in the liraglutide arms compared to placebo. SCALE (Type 2 Diabetes) and
SCALE (Insulin), which both included participants with obesity and diabetes mellitus, exhibited
higher rates of serious adverse events compared to trials in the SCALE clinical trial program, which
evaluated participants with obesity without diabetes mellitus.
42,44
Across all SCALE trials, there
were generally higher rates of gallbladder-related and pancreatic adverse events in the intervention
arm compared to placebo. See Table 3.16 below for detailed harms results.

©Institute for Clinical and Economic Review, 2022 Page 27
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 3.16. Harms in Key Trials of Liraglutide for the Management of Obesity and Obesity with Diabetes Mellitus
40-45,48,50-52
SCALE
Maintenance
SCALE
Sleep Apnea
SCALE
Obesity and
Pre-Diabetes
SCALE
IBT
SCALE
Type 2 Diabetes*
SCALE
Insulin*
Study Arms
PBO
LIR
PBO
LIR
PBO
LIR
PBO
LIR
PBO
LIR
PBO
LIR
N
210
212
179
176
1,242
2,481
140
142
212
422
197
195
Any AE, n (%)
186
(88.6)
194
(91.5)
124
(69.3)
141
(80.1)
786
(63.3)
1,992
(80.3)
124
(88.6)
136
(95.8)
182
(85.8)
392
(92.9)
175
(88.8)
180
(92.3)
SAE, n (%) 5 (2.4) 9 (4.3) 6 (3.4) 6 (3.4) 62 (5)
154
(6.2)
2 (1.4) 6 (4.2) 21 (9.9)
52
(12.3)
19 (9.6) 16 (8.2)
AE Leading to
Discontinuation, n (%)
18 (8.6) 18 (8.5) NR NR 47 (3.8)
240
(9.7)
6 (4.3) 12 (8.5) 7 (3.3) 39 (9.2) 6 (3) 15 (7.7)
Nausea, n (%)
36
(17.1)
101
(47.6)
12 (6.7)
47
(26.7)
183
(14.7)
997
(40.2)
25
(17.9)
68
(47.9)
29
(13.7)
138
(32.7)
23
(11.7)
58
(29.7)
Constipation, n (%)
26
(12.4)
57
(26.9)
6 (3.4)
21
(11.9)
108
(8.7)
495 (20)
26
(18.6)
43
(30.3)
13 (6.1)
68
(16.1)
17 (8.6)
28
(14.4)
Diarrhea, n (%)
26
(12.4)
38
(17.9)
14 (7.8)
29
(16.5)
115
(9.3)
518
(20.9)
23
(16.4)
31
(21.8)
27
(12.7)
108
(25.6)
30
(15.2)
45
(23.1)
AE: adverse event, LIR: liraglutide, n: number, N: total number, NR: not reported, PBO: placebo, SAE: serious adverse event
*Included participants with obesity and diabetes mellitus.

©Institute for Clinical and Economic Review, 2022 Page 28
Evidence Report – Medications for Obesity Management Return to Table of Contents
Phentermine/Topiramate
Adverse events of any cause in the EQUIP, EQUATE, and CONQUER trials were mostly mild to
moderate in severity. Rates of any adverse events were relatively high among all arms (73-86%),
with highest rates in the high-dose phentermine/topiramate arm, followed by the low-dose
phentermine/topiramate arm, and the placebo arm (Table 3.17).
54-56,58
Adverse reactions that
occurred more frequently in the high-dose and low-dose phentermine/topiramate treatment
groups included paresthesia, nausea, dry mouth, constipation, and headache. EQUIP and CONQUER
also assessed psychiatric adverse events, such as insomnia, anxiety, and depression, which were
more common in the high-dose and low-dose phentermine/topiramate arms,
54,56
with the
exception of depression in the CONQUER trial, where the incidence of depression in the low-dose
intervention arm (3%) was similar to the placebo arm (3.2%).
58
Serious adverse reactions were relatively low among all trials and arms (0-6%). In the EQUIP trial,
participants in all arms reported serious adverse events at the same rate (2.5%),
56
while in the
EQUATE trial, more participants in the high-dose treatment arm (1.9%) and low-dose treatment arm
(0.9%) reported more serious adverse events than in the placebo arm (0%).
54
In the CONQUER trial,
incidence of serious adverse events was 3.7% in the high-dose phentermine/topiramate arm, 6% in
the low-dose phentermine/topiramate arm, and 3.2% in the placebo arm.
58
Serious adverse events
that occurred infrequently in the phentermine/topiramate arms were chest pain, nephrolithiasis,
appendicitis, blurred vision, humerus fracture, and myelogenous leukemia. Among all trials,
discontinuation due to adverse events occurred most frequently in the high-dose arm (16-21%),
followed by the low-dose arm (9-15%), and placebo (7-8%). See Table 3.17 for more details on
harms.

©Institute for Clinical and Economic Review, 2022 Page 29
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 3.17. Harms in Key Trials of Phentermine/Topiramate for the Management of Obesity and
Obesity with Diabetes Mellitus
EQUIP
EQUATE
CONQUER (Diabetes Subgroup)*
Study Arms PBO
P/T
(high)
PBO
P/T
(low)
P/T
(high)
PBO P/T (low)
P/T
(high)
N
513
511
109
106
108
157
67
164
Any AE, n (%)
374
(72.9)
432
(84.5)
87
(79.8)
85
(80.2)
90
(83.3)
125
(79.6)
54 (80.6) 141 (86)
SAE, n (%)
13 (2.5)
13 (2.5)
0 (0)
1 (0.9)
2 (1.9)
5 (3.2)
4 (6)
6 (3.7)
AE Leading to
Disc., n (%)
43 (8.4) 82 (16) 8 (7.3)
16
(15.1)
23
(23.1)
13 (8.3) 6 (9) 31 (18.9)
Paresthesia, n (%) 10 (1.9) 96 (18.8) 4 (3.7) 17 (16)
25
(23.1)
6 (3.8) 5 (7.5) 29 (17.7)
Dry Mouth, n (%) 19 (3.7) 87 (17) 0 (0)
14
(13.2)
20
(18.5)
6 (3.8) 5 (7.5) 22 (13.4)
Headache, n (%)
52
(10.1)
61 (11.9)
14
(12.8)
16
(15.1)
17
(15.7)
9 (5.7) 3 (4.5) 18 (11)
Constipation, n (%) 35 (6.8) 72 (14.1) 9 (8.3) 7 (6.6)
17
(15.7)
10 (6.4) 10 (14.9) 29 (17.7)
Nausea, n (%)
24 (4.7)
37 (7.2)
5 (4.6)
9 (8.5)
8 (7.4)
8 (5.1)
1 (1.5)
13 (7.9)
Insomnia, n (%) 25 (4.9) 40 (7.8) 6 (5.5)
13
(12.3)
11
(10.2)
8 (5.1) 5 (7.5) 23 (14)
Anxiety, n (%)
6 (1.2)
19 (3.7)
NR
NR
NR
NR
NR
NR
Depression, n (%)
6 (1.2)
24 (4.7)
NR
NR
NR
5 (3.2)
2 (3)
10 (6.1)
AE: adverse event, Disc.: discontinuation, n: number, N: total number, NR: not reported, PBO: placebo, P/T:
phentermine/topiramate, SAE: serious adverse event
*Included participants with obesity and diabetes mellitus.
Bupropion/Naltrexone
Any adverse events in COR-I, COR-II, COR-BMOD, and COR Diabetes occurred at a higher rate in the
bupropion/naltrexone arms (83-90%) than in placebo (67-75%).
59,61,63,65,66
Nausea, dry mouth,
headache, constipation, and upper respiratory tract infection occurred more frequently in the
treatment arms compared to placebo. Occurrence of psychiatric events, such as insomnia, anxiety,
depression, and stress, varied among all trials. Insomnia occurred more frequently in the
bupropion/naltrexone group versus placebo in COR-I, COR-II, and COR-BMOD. Rates of anxiety
were higher in the intervention arms than in placebo arms in COR-II and COR-BMOD but were lower
than in the placebo arm in COR-I (Table 3.18). Depression occurred at a higher rate in the
treatment groups in all studies except COR-BMOD. Participants in the bupropion/naltrexone group
in COR-BMOD also experienced less stress than participants in the placebo arm.
In COR-I, COR-II and COR-BMOD, serious adverse events were more frequent in the intervention
arms (2-4%) versus the placebo arm (1%).
61-66
In the COR Diabetes trial assessing participants with
obesity and diabetes mellitus, serious adverse events were more common in the placebo arm
(4.7%) than in the treatment arm (3.9%).
59,60
Serious adverse events that occurred infrequently in

©Institute for Clinical and Economic Review, 2022 Page 30
Evidence Report – Medications for Obesity Management Return to Table of Contents
the bupropion/naltrexone arm were cholecystitis, cardiac failure, and seizures. Discontinuation due
to adverse events occurred more frequently in the bupropion/naltrexone arms (20-29%) than in the
placebo arms across the trials (10-15%). See Table 3.18 below for more details on harms.

©Institute for Clinical and Economic Review, 2022 Page 31
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 3.18. Harms in Key Trials of Bupropion/Naltrexone for the Management of Obesity and Obesity with Diabetes Mellitus
59-66
COR-I
COR-II
COR-BMOD
COR Diabetes*
Study Arms
PBO
B/N
PBO
B/N
PBO
B/N
PBO
B/N
N
569
573
492
992
200
584
169
333
Any AE, n (%)
390 (68.5)
476 (83.1)
370 (75.2)
852 (85.9)
133 (66.5)
487 (83.4)
144 (85.2)
301 (90.4)
SAE, n (%)
8 (1.4)
9 (1.6)
7 (1.4)
21 (2.1)
1 (0.5)
22 (3.8)
13 (4.7)
8 (3.9)
AE leading to
Disc., n (%)
56 (9.8) 112 (19.5) 68 (13.8) 241 (24.3) 25 (12.4) 150 (25.4) 26 (15.4) 98 (29.4)
Death, n (%)
0 (0)
1 (0.2)
NR
NR
0 (0)
0 (0)
NR
NR
Dry mouth, n (%)
11 (1.9)
43 (7.5)
13 (2.6)
90 (9.1)
6 (3)
47 (8)
5 (3)
21 (6.3)
Headache, n (%)
53 (9.3)
79 (13.8)
43 (8.7)
174 (17.5)
35 (17.5)
139 (23.8)
15 (8.9)
46 (13.8)
Constipation, n
(%)
32 (5.6) 90 (15.7) 35 (7.1) 189 (19.1) 28 (14) 141 (24.1) 12 (7.1) 59 (17.7)
URTI, n (%)
64 (11.2)
57 (9.9)
55 (11.2)
86 (8.7)
NR
NR
16 (9.5)
26 (7.8)
Nausea, n (%)
30 (5.3)
171 (29.8)
34 (6.9)
290 (29.2)
21 (10.5)
199 (34.1)
12 (7.1)
141 (42.3)
Insomnia, n (%)
29 (5.1)
43 (7.5)
33 (6.7)
97 (9.8)
12 (6)
51 (8.7)
9 (5.3)
37 (11.1)
Anxiety, n (%)
12 (2.1)
9 (1.6)
21 (4.3)
48 (4.8)
7 (3.5)
30 (5.1)
2 (1.2)
18 (5.4)
Depression, n (%)
6 (1.1)
3 (0.5)
8 (1.6)
13 (1.3)
5 (2.5)
2 (0.3)
3 (1.8)
2 (0.6)
Stress, n (%)
NR
NR
NR
NR
4 (2)
3 (0.5)
NR
NR
AE: adverse event, B/N: bupropion/naltrexone, Disc.: discontinuation, n: number, N: total number, NR: not reported, PBO: placebo, SAE: serious adverse event,
URTI: upper respiratory tract infection
*Included participants with obesity and diabetes mellitus.
†N=202.
‡N=591.

©Institute for Clinical and Economic Review, 2022 Page 32
Evidence Report – Medications for Obesity Management Return to Table of Contents
NMA Results of Discontinuation
For the outcome of discontinuation due to adverse events, we conducted an NMA of trials including
participants with obesity alone and excluded trials of participants with obesity and diabetes
mellitus. The discontinuation NMA included more trials than in the efficacy NMAs as we did not
exclude trials that included IBT programs as part of the lifestyle component of the trial arms. The
NMA of discontinuation due to adverse events is reported below, and the network diagram is
presented in the Supplement
.
Participants with Obesity Alone
For the trials of the medications conducted in participants with obesity without diabetes mellitus
and reported discontinuation due to adverse events, we present the results of the unadjusted
random effects model in Table 3.19, given its better fit for the model compared to the baseline risk
adjusted model. Discontinuation rates due to adverse events were higher for all medications
compared to placebo. Semaglutide may have lower discontinuation rates than liraglutide,
phentermine/topiramate, and bupropion/naltrexone, however, these results were not statistically
significant (Table 3.19).
Table 3.19. NMA Results of Medications for the Management of Obesity, Odds Ratio of
Discontinuation Rates due to Adverse Events (95% CI)
Semaglutide
0.7 (0.3-1.3) Liraglutide
0.8 (0.3-1.5) 1.1 (0.5-2.2)
Bupropion/
Naltrexone
0.7 (0.2-1.5) 1.0 (0.4-2.3) 0.9 (0.4-2.1)
Phentermine/
Topiramate*
1.7 (0.9-2.8) 2.4 (1.4-4.0) 2.2 (1.3-3.7) 2.4 (1.3-5.2)
Placebo
Legend: Each box represents the estimated odds ratio of discontinuation due to adverse events and 95% credible
interval for the combined direct and indirect comparisons between two medications or one medication and
placebo. Estimates in bold indicate the 95% credible interval does not contain 1.

©Institute for Clinical and Economic Review, 2022 Page 33
Evidence Report – Medications for Obesity Management Return to Table of Contents
Subgroup Analyses and Heterogeneity
We sought evidence on obesity management in subgroups of interest such as in individuals with
higher or lower baseline BMI, pre-diabetes, or previous weight loss surgery. We also sought
evidence comparing obesity management based on sex and race/ethnicity. However, data were
generally not available or were provided to ICER as confidential. In the STEP 1 and 2 trials of
semaglutide, SCALE Obesity and Pre-Diabetes trial of liraglutide, and EQUIP trial of
phentermine/topiramate in adults with obesity, percentage weight loss was generally consistent
across BMI subgroups corresponding to obesity classes I/II/III, suggesting a benefit across the range
of obesity severity included in these trials. In a post-hoc analysis of the STEP 1, 3, and 4 trials of
semaglutide (which enrolled 40-50% of participants with pre-diabetes), improvements in A1C and
blood glucose were comparable or better among participants with pre-diabetes than among the
overall study population, suggesting a benefit in glycemic status consistent with the drug’s
mechanism of action.
39
In abstract reports from the STEP 1, 2 and 3 trials of semaglutide, race and ethnicity were not
associated with weight loss outcomes, though female gender was reported to be associated with
greater weight loss.
32,69,70
In analysis of pooled data from four SCALE trials, mean change in weight
loss for liraglutide compared to placebo for White, Black/African American and Asian patients were
-5.3%, -4.8% and -4.0%, respectively.
71
The CONQUER trial provided subgroup data on sex, race,
and ethnicity in the Supplement. In participants receiving phentermine/topiramate high- and low-
dose treatment, weight loss in this trial was greater in females than males (11.0% vs. 9.1% and 8.8%
vs. 7.5%, respectively, in females vs. males). Additionally, participants in the
phentermine/topiramate arms who were Black experienced a similar amount of weight loss
compared to participants who were non-Black (9.7% vs. 10.5% and 9.7% vs. 8.5%, respectively).
53
Uncertainty and Controversies
Though pharmacy claims data suggest that many individuals who take medications for weight loss
do not use them for long periods of time, experts and patients we spoke with highlighted that
weight regain after stopping treatment is common.
72
This points to the need for long-term use of
these medications. All key trials reported outcomes over approximately one year follow-up. Few
comparative trials have examined longer-term outcomes making the benefits and harms of these
medications over prolonged periods uncertain. For individuals without diabetes mellitus, heart
disease, arthritis, sleep apnea, or cancer, studies have not shown whether weight loss prevents
disease morbidity and mortality. Studies of treatments for obesity in individuals undergoing weight
loss surgery for severe obesity demonstrate decreased incidence of cardiovascular- and cancer-
related outcomes and lower mortality.
4,26,27
However, these results primarily come from
observational studies and the benefit in individuals without diabetes mellitus or lower baseline

©Institute for Clinical and Economic Review, 2022 Page 34
Evidence Report – Medications for Obesity Management Return to Table of Contents
weights is less clear. Thus, there is a need for studies examining long-term outcomes in individuals
without diabetes mellitus who are chronically using weight loss medications.
73
We primarily used indirect quantitative methods (NMAs) to compare semaglutide, liraglutide,
phentermine/topiramate, and bupropion/naltrexone to each other because there was only a single
head-to-head study of semaglutide and liraglutide. Differences in study populations, lifestyle
interventions offered, and escalation schedules that led to different follow-up intervals all
contribute to indirect analyses having more uncertainty than if the therapies had been compared
directly in randomized controlled trials.
All of the pivotal Phase III randomized controlled trials compared the active agents to placebo
among patients receiving lifestyle interventions. As a result, the studies assessed the additive
benefit of the drugs in addition to lifestyle interventions that varied among the studies. Because we
expect that medications when used in routine clinical practice will more commonly be given with
less intensive lifestyle interventions, our primary analyses included trials with standard lifestyle
interventions and may represent the best evidence for the efficacy of the active therapies. Other
trials compared drugs to placebo along with more intensive lifestyle interventions that included IBT
or structured meal programs. These trials also demonstrated benefit of the drugs compared to
placebo, but in general, the amount of weight loss was slightly less than seen in the trials with
standard lifestyle interventions.
These trials examined the relative benefits of the individual and fixed dose combination agents as
single interventions. The drugs that make up the phentermine/topiramate and
bupropion/naltrexone combinations are also approved for other indications as individual drugs at
somewhat different doses. We heard from experts that these individual drugs are used singly or in
various combinations in an “off-label” manner. Clinicians said such use may mitigate side effects
and be less costly to patients. Semaglutide and liraglutide are FDA-approved for treatment of
diabetes mellitus at lower doses, and while these doses may be associated with less weight loss
than the doses used in our primary outcome analyses, these lower doses may be used, especially in
those with co-existing diabetes mellitus, because they may be better covered by insurers and result
in fewer out-of-pocket expenses to patients.
We only compared results of individual drugs or approved fixed dose combinations. Using multiple
drugs that target different mechanisms or newer drugs that have more than one mechanism of
action (e.g., tirzepatide) may achieve synergistic effects and provide greater weight loss. In addition
to their weight loss properties, semaglutide and liraglutide as GLP-1 receptor agonists have also
been shown to decrease blood sugar in individuals with pre-diabetes and diabetes mellitus, and to
decrease major adverse cardiovascular events among individuals with diabetes mellitus. It is not
known whether GLP-1 receptor agonists provide benefits to individuals with obesity that go beyond
their weight loss effects compared to other approved weight loss drugs with different mechanisms

©Institute for Clinical and Economic Review, 2022 Page 35
Evidence Report – Medications for Obesity Management Return to Table of Contents
of action. At present, this remains uncertain for individuals without diabetes mellitus using GLP-1
receptor agonists for weight loss and warrants future investigation.
There is limited information available about the relative benefits and harms of these drugs in
important subgroups including patients with lower BMIs. Similarly, for those with BMIs of greater
than 40 where weight loss surgery is an option, the relative benefits and harms of these drugs
compared to weight loss surgery is uncertain. Moreover, experts discussed that these medications
are being used in individuals after weight loss surgery to treat or prevent weight regain, and the
effects of their use here is also uncertain. For women of childbearing age, there is a lack of data on
the potential impact of medications for weight reduction on fertility, maternal morbidity and
mortality, and infant health.
Trials of weight loss medications include populations that are underrepresented in terms of the
percentage of men and minority groups. Weight reductions seen in these trials among men and
women appeared similar. Since most trials included mostly White patients and given the large
impact of obesity in Black Americans and other racial and ethnic groups, there is a need for more
studies evaluating the outcomes of the various medications in these populations. For example, a
post-hoc analysis of liraglutide trials showed similar weight reduction across racial and ethnic
groups.
74


©Institute for Clinical and Economic Review, 2022 Page 37
Evidence Report – Medications for Obesity Management Return to Table of Contents
Results from the clinical trials and from our NMAs demonstrate that semaglutide, liraglutide,
phentermine/topiramate, and bupropion/naltrexone, when used as adjuncts to usual care, improve
weight loss outcomes of patients with obesity compared to usual care alone (e.g., standard lifestyle
management). The magnitude of the weight loss appears to be greater for semaglutide and
phentermine/topiramate than for liraglutide and bupropion/naltrexone based on the one head-to-
head trial of semaglutide and liraglutide and our indirect NMA results. Other outcomes show that
semaglutide and liraglutide improved blood sugar, blood pressure, and physical function compared
to usual care. Blood pressure was lower with phentermine/topiramate than usual care. Blood
sugar results were not reported in the phentermine/topiramate and bupropion/naltrexone trials for
patients without diabetes mellitus.
Semaglutide, liraglutide, phentermine/topiramate, and bupropion/naltrexone all had common
adverse events, but few serious harms were reported in the trials. Discontinuation due to adverse
events was higher for each intervention compared to placebo. Patients taking liraglutide,
phentermine/topiramate, and bupropion/naltrexone may have higher discontinuation rates due to
adverse events than for semaglutide.
There is uncertainty about the relative benefit and safety among the four medications due to
differences in the trials with regards to their size, patient characteristics, concomitant lifestyle
interventions, outcomes assessed, and duration of follow-up that the indirect nature of the NMAs
do not fully capture. For all of the drugs, there is a lack of long-term efficacy and safety data that
includes whether sustained weight loss leads to decreased clinical endpoints and if weight regain
may occur over time despite continued therapy as has been seen with weight loss surgery.
75
Differences among the medications in their mechanisms of action may also lead to differences in
clinical endpoints, such as heart disease, that go beyond their effects on weight loss. For example,
semaglutide and liraglutide have been shown to reduce cardiovascular disease endpoints in
patients with type 2 diabetes mellitus,
76
but this is uncertain for individuals with obesity without
diabetes mellitus.
In summary, for adults with obesity who have not had sufficient weight loss with lifestyle
interventions alone and are interested trying weight loss medications, we assessed the benefits and
harms of these four medications added to lifestyle modification compared to standard lifestyle
modification alone and to each other. As such:
• We consider the evidence for the net health benefit of semaglutide added to lifestyle
modification compared to lifestyle modification alone to be incremental or better (“B+”),
demonstrating a moderate certainty of a small or substantial net health benefit, with high
certainty of at least a small net health benefit. This rating is based upon demonstration of
substantial short-term weight loss from multiple high-quality studies with few serious
harms, but higher rates of discontinuation due to adverse events than placebo, uncertainty

©Institute for Clinical and Economic Review, 2022 Page 38
Evidence Report – Medications for Obesity Management Return to Table of Contents
about long-term ability to sustain weight loss, and whether the degree of weight loss in this
population results in improved clinical outcomes.
• We consider the evidence for the net health benefit of liraglutide added to lifestyle
modification compared to lifestyle modification alone to be incremental (“B”),
demonstrating a high certainty of a small net health benefit. This rating is based upon
demonstration of small to moderate short-term weight loss from multiple high-quality
studies with few serious harms; our expectation is that even if the weight loss were
sustained, the benefits would only be incremental.
• We consider the evidence for the net health benefit of phentermine/topiramate added to
lifestyle modification compared to lifestyle modification alone to be comparable or better
(“C++”), demonstrating a moderate certainty of a comparable, small, or substantial net
health benefit, with high certainty of at least a comparable net health benefit. This rating is
based upon demonstration of moderate to substantial short-term weight loss from a limited
number of trials with few serious harms, but higher rates of discontinuation due to adverse
events than placebo, uncertainty about long-term ability to sustain weight loss, and
whether the degree of weight loss seen translates into improved clinical outcomes given the
limited data from clinical process measures.
• We consider the evidence for the net health benefit of bupropion/naltrexone added to
lifestyle modification compared to lifestyle modification alone to be comparable or
incremental (“C+”), demonstrating a moderate certainty of a comparable or small net health
benefit, with high certainty of at least a comparable net health benefit. This rating is based
upon demonstration of small to moderate short-term weight loss from several trials with
few serious harms, but higher rates of discontinuation due to adverse events than placebo,
uncertainty about long-term ability to sustain weight loss, and whether the degree of
weight loss seen translates into improved clinical outcomes given the limited data from
clinical process measures.
• We consider the evidence for the net health benefit of semaglutide compared to liraglutide
and phentermine/topiramate to be comparable or incremental (“C+”), and compared to
bupropion/naltrexone to be comparable or better (“C++”). The rating comparing
semaglutide to liraglutide is based upon greater weight loss and fewer adverse reactions
leading to discontinuation with semaglutide, but uncertainty about long-term ability to
sustain weight loss and, given the same mechanism of action, whether the incremental
amount of weight loss results in improved clinical outcomes in this population. The rating
comparing semaglutide to phentermine/topiramate is based upon similar weight loss and
fewer adverse reactions leading to discontinuation, but differences in the number and
quality of the trials, differences in mechanisms of action that may impact clinical outcomes,
and uncertainty about long-term ability to sustain weight loss. The rating comparing

©Institute for Clinical and Economic Review, 2022 Page 39
Evidence Report – Medications for Obesity Management Return to Table of Contents
semaglutide to bupropion/naltrexone is based upon greater weight loss and fewer adverse
reactions leading to discontinuation with semaglutide, but differences in mechanisms of
action that may impact clinical outcomes, and uncertainty about long-term ability to sustain
weight loss.
Table 3.20. Evidence Ratings of Medications for Obesity Management
Treatment
Comparator
Evidence Rating
Semaglutide
Lifestyle modification
B+
Liraglutide
Lifestyle modification
B
Phentermine/Topiramate
Lifestyle modification
C++
Bupropion/Naltrexone
Lifestyle modification
C+
Semaglutide
Liraglutide
C+
Phentermine/topiramate
C+
Bupropion/naltrexone
C++

©Institute for Clinical and Economic Review, 2022 Page 40
Evidence Report – Medications for Obesity Management Return to Table of Contents
4. Long-Term Cost Effectiveness
4.1. Methods Overview
The primary aim of this analysis was to estimate the cost effectiveness of semaglutide, liraglutide,
phentermine/topiramate, and bupropion/naltrexone plus lifestyle modification compared to
standard lifestyle modification alone, and to each other, for life-long weight management in the
treatment of overweight and obesity. The base-case analysis comparatively evaluated each therapy
option in a cohort of patients consistent with clinical trials and real-world evidence. Patients were
80% female with an average age of 45 years, BMI of 38 kg/m
2
, SBP of 125 mmHg, and HbA1C of
5.7% without confirmed diabetes mellitus. Additional scenarios were evaluated as described in
Section 4.3.
We built a Markov state transition model informed by key clinical trials, prior relevant economic
models, systematic literature reviews, and input from a diverse set of stakeholders (patients,
advocacy groups, clinicians, payers, researchers, and manufacturers of these agents) from the
health care sector perspective (i.e., focused on direct medical care costs) using a lifetime time
horizon. The model cycle length was one year, and all costs and outcomes were discounted at a
rate of 3% per year.
As shown in the model diagram below (Figure 4.1), simulated patients entered the model through
their medication regimen to the initial Markov state “No diabetes mellitus.” From the first cycle
onward, patients could remain in the starting state, or transition to any of four non-heart-failure
cardiovascular comorbid health states (myocardial infarction, stroke, stroke plus myocardial
infarction, or other cardiovascular disease) with or without developing diabetes mellitus. Other
cardiovascular disease included peripheral artery disease, angina, and transient ischemic attack.
Myocardial infarction was a prerequisite to developing heart failure because of the strong causal
association between obesity and heart failure mediated by myocardial changes.
77
The model
assumed all patients with hypertension were optimally controlled with antihypertensive
medication. As it is uncertain whether obesity is an independent risk factor for non-ischemic heart
failure in patients with controlled blood pressure, we opted to not account for any additional risk of
heart failure through alternate pathways. At any state in the model, patients could transition to the
terminal “Death” state.

©Institute for Clinical and Economic Review, 2022 Page 41
Evidence Report – Medications for Obesity Management Return to Table of Contents
Figure 4.1. Model Diagram
CVD: cardiovascular disease, DM: diabetes mellitus, HF: heart failure, LM: lifestyle management, LIR: liraglutide,
MI: myocardial infarction, B/N: bupropion/naltrexone, P/T: phentermine/topiramate, SEM: semaglutide
Average BMI reduction with therapy was the primary factor used to estimate differences in
cardiovascular comorbidity and risk of progression to diabetes mellitus. The annual risk of
developing cardiovascular conditions at the beginning of each cycle was calculated using a
published risk equation model based on BMI, presence of diabetes mellitus, population
demographics, and clinical characteristics. Specifically, the 2013 American College of Cardiology/
American Heart Association (ACC/AHA) guideline risk equation was used to calculate the 10-year
risk of non-heart-failure cardiovascular conditions.
78
The resulting 10-year risks were then used to
calculate the annual probability of a cardiovascular event and were updated in each cycle of the
model using the equation []=1−
(−
t)
. BMI was included as a time-varying input in the risk
calculation for each cycle.
The risk of a cardiovascular event was calculated for each combination of patient factors (e.g., male
vs. female, smokers vs. nonsmokers, and active hypertension treatment vs. no hypertension
treatment, diagnosis of diabetes mellitus vs. no diabetes mellitus, age, and BMI) and the weighted
average was used to calculate overall risk. Cardiovascular event risks were then further stratified

©Institute for Clinical and Economic Review, 2022 Page 42
Evidence Report – Medications for Obesity Management Return to Table of Contents
into specific stroke, myocardial infarction, and other cardiovascular disease event probabilities
given the proportion of each condition observed in a US population.
79-82
Our model captured the impact of weight loss in delaying the onset of diabetes mellitus. In
addition, the HbA1C-lowering effect of semaglutide and liraglutide was expected to further delay
the onset of diabetes mellitus.
83,84
Therefore, we calculated the annual incidence of diabetes
mellitus for each cycle using BMI and HbA1C data.
85
Furthermore, weight loss from medication
therapy may result in hypertension remission. We therefore incorporated an association between
BMI and hypertension to allow for a decreased prevalence of hypertension as BMI decreased.
86,87
Although we did not explicitly include some conditions known to be associated with obesity, the
anticipated benefit of weight loss in reducing the onset of such conditions was implicitly captured.
For example, the impact of weight loss on sleep apnea is captured by the mortality benefits
mediated by cardiovascular conditions. Chronic kidney disease was not included as a separate
Markov state in the base-case simulation as most chronic kidney disease results from diabetes
mellitus or hypertension. By including costs and quality of life changes from studies with a broad
selection of patients with diabetes mellitus, we implicitly addressed the influence of chronic kidney
disease in the model. Chronic kidney disease resulting from hypertension was not captured in the
base case, as we assumed that hypertension management was optimal in patients with and without
weight loss. However, a scenario analysis (described below as “Comorbidity X”) captured the
potential impact of weight-related chronic kidney disease (and cancer) on the cost effectiveness of
medications for obesity management. Improvements in lipids were not explicitly included in the
model. The ACC/AHA risk equations for cardiovascular risk account for either changes in weight or
LDL, but not both simultaneously. Therefore, including changes to lipids in the model would likely
double count the cardiovascular benefits from treatment. Supplement Section E1
details additional
rationale behind our choice of health states in the base case.
Health gains in the model were mainly derived from increased utility in those with improved BMI
associated with enhanced daily functioning, decreased risk of developing diabetes
mellitus/cardiovascular disease, and reduced complications/comorbidities. The estimated utility
gains from enhanced daily functioning included improvements in conditions such as sleep apnea,
gastroesophageal reflux disease, and osteoarthritis as well as improved mobility and self-image.

©Institute for Clinical and Economic Review, 2022 Page 43
Evidence Report – Medications for Obesity Management Return to Table of Contents
Scenario Analyses
In order to address several uncertainties, we conducted multiple scenario analyses:
• Societal perspective (including labor costs)
• Evaluation of patients with a starting BMI of ≥40 kg/m
2
(i.e., weight class III with average
BMI of 42.5 and 47.5 kg/m
2
)
• Use of generic phentermine/topiramate and bupropion/naltrexone
• Patient population consisting of a similar proportion of men and women (50:50)
• Comorbidity X scenario individually assessing the potential impact of BMI change resulting
from medications for obesity management on chronic kidney disease and cancer
• Evaluation of a “Drug X” with the effect on weight loss seen in the SUPPORT 1 trial of
tirzepatide and pricing of semaglutide for overweight and obesity and effects on blood
pressure and diabetes mellitus similar to semaglutide.
Further details on the economic modeling methods used are available in Supplement E.
Based on public comment, the following changes were made:
1) Updated the discontinuation rate from estimates for serious adverse event rates from
clinical trials to values reported in the NMA, which estimated adverse events leading to
discontinuation
2) Included the full results of two scenario analyses that had been omitted from the results
section of the Draft Evidence Report. These scenarios were: a) Evaluation of patients with a
starting BMI of ≥40 kg/m
2
(i.e., weight class III with average BMI of 42.5 and 47.5 kg/m
2
);
and b) Patient population consisting of a similar proportion of men and women (50:50)
3) Removed the direct influence of bupropion/naltrexone on HbA1C; cardiovascular benefits of
bupropion/naltrexone were made through weight reduction.
The following scenario analyses were included in the Model Analysis Plan but were either changed
to sensitivity analyses or were not conducted:
1) Weight regain scenario: Scenarios evaluating short-term treatment followed by weight-
regain were evaluated and removed due to a potential overestimation of benefits
2) Subgroup of patients who respond to the lower maintenance dose of
phentermine/topiramate: We chose to only model the maximum dose and effect of Qsymia
with the understanding that providers would attempt to maximize weight loss, provided
patients tolerated treatment
3) Patients with diabetes mellitus at baseline: Since the effectiveness of semaglutide and
liraglutide have previously been evaluated by ICER, our model was designed to evaluate the
impact of weight management in patients without diabetes. We assumed that for patients

©Institute for Clinical and Economic Review, 2022 Page 44
Evidence Report – Medications for Obesity Management Return to Table of Contents
with diabetes, there would be no difference in the management of diabetes (i.e., HbA1C
levels) between patients on different medications or lifestyle management alone for obesity
management. Therefore, with the exception of delays to diabetes onset resulting from the
effects of the drugs on HbA1C, we did not include the impact of treatments on HbA1C
4) Optimistic and conservative assumptions regarding the benefit of treatment: We tested the
optimistic and conservative weight reduction scenarios in one-way sensitivity analyses
4.2. Key Model Assumptions and Inputs
Model Assumptions
Several assumptions were required to estimate the cost effectiveness of treatments for obesity.
These assumptions were based on clinical expert opinion, a review of the available evidence and
published models, and the investigators’ experience with developing similar models. The key model
assumptions and rationales for each assumption are listed below in Table 4.1. Additional model
assumptions are described in the Supplement
.

©Institute for Clinical and Economic Review, 2022 Page 45
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 4.1. Key Model Assumptions
Assumption
Rationale
Cardiovascular risk
equations provide the best
estimate of treatment
benefit on cardiovascular
outcomes
Certain drug treatments may have benefits unrelated to weight loss achieved
or changes in HbA1C. In the absence of strong evidence for the effects of
medications on cardiovascular risk in patients with obesity and without
diabetes mellitus, we did not include such a benefit. Should evidence emerge
supporting additional benefits, the model can be updated to include these
benefits. The potential benefits on cardiovascular outcomes of delays in
diabetes mellitus onset from therapies that directly reduce A1C, beyond
those associated with weight reduction, provided sufficient evidence exists,
will be considered in the model.
Patients continue to receive
the intervention or lifestyle
modification throughout
the model time horizon
Expert opinion suggests that since obesity is increasingly considered as a
chronic metabolic disease requiring long-term management to affect
outcomes, long-term treatment is required for most individuals. After
stopping therapy, weight regain is common. Further, repeated fluctuations in
body weight, i.e., “weight cycling,” is associated with adverse health
outcomes.
Treatment discontinuation
is included in the model
prior to the first model
cycle; longitudinal changes
in the persistence and
adherence to medications
were not considered in the
model
Including the impact of poor long-term persistence requires the addition of
several “discontinuation” health states, thereby increasing model complexity.
Further, there is no information on the impact of short-term treatment on
cardiovascular outcomes, especially after discontinuation of treatment.
Proportion of actively
treated hypertension is a
function of BMI without a
significant influence on the
incremental cost-
effectiveness ratio
BMI significantly influences the proportion of patients in need of
hypertension treatment. Assuming hypertension treatment effectively
manages overall SBP, average SBP would be similar across the treatment
strategies over the model time horizon. The cost of hypertension medication
is small and is therefore unlikely to influence the incremental cost-
effectiveness ratio.
In patients with
hypertension, blood
pressure is equally well
managed across all weight
loss treatments
Weight loss treatments may affect blood pressure differently. The impact of
treatments on reducing the likelihood of needing treatment for hypertension
was included in the model. For those who continued to require treatment for
hypertension, we assumed that all patients would have similar outcomes
related to hypertension treatment.
HbA1C: glycated hemoglobin, SBP: systolic blood pressure
Model Inputs
The key model inputs are listed in Table 4.2. The clinical inputs for the model were weighted over
time and by associated probabilities of cardiovascular disease (myocardial infarction, stroke, other
cardiovascular disease), heart failure, and diabetes mellitus. Weight change resulting from
treatment was determined from an NMA of trials conducted as part of this review. The risk of
myocardial infarction, stroke, and other cardiovascular disease was obtained from a risk equation
model.
87-89
Risk of heart failure and diabetes mellitus was determined from a systematic review of
the literature and published risk equations.
85,90-94

©Institute for Clinical and Economic Review, 2022 Page 46
Evidence Report – Medications for Obesity Management Return to Table of Contents
BMI and weight trajectory over time were used as model inputs to assess cardiovascular risk.
Percent weight change (and thus BMI change, assuming no change in height) from baseline at year
one and maximum percent weight change by the end of the second year were incorporated into the
model. We assumed patients received the maintenance dose continuously, the medication
maintained long-term effectiveness, and there was no additional weight change beyond the
maximum weight reduction until the end of the model time horizon in the base case.
The impact of weight loss on mortality was incorporated as reduction of fatal cardiovascular events,
as estimated from a review of existing literature and a direct extraction of general population all-
cause mortality from the Human Mortality Database US-specific life tables.
95,96

©Institute for Clinical and Economic Review, 2022 Page 47
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 4.2. Key Model Inputs*
Parameter
Input
Source
Clinical Inputs
Absolute Difference in % Weight Change, SEM vs. LSM
-13.7%
ICER NMA, Table 3.11
Absolute Difference in HbA1C Change, SEM vs. LSM
-0.30
STEP 1
34
Absolute Difference in % Weight Change, LIR vs. LSM
-5.0%
ICER NMA, Table 3.11
Absolute Difference in HbA1C Change, LIR vs. LSM
-0.20
SCALE (Maintenance)
41
Absolute Difference in % Weight Change, P/T vs. LSM
-9.1%
ICER NMA, Table 3.11
Absolute Difference in HbA1C Change, P/T vs. LSM
0.00
EQUATE
53,57,58
Absolute Difference in % Weight Change, B/N vs. LSM
-4.6%
ICER NMA, Table 3.11
Absolute Difference in HbA1C Change, B/N vs. LSM
0.00
61,65
Baseline Risk of CV Event, Female Non-Smoker without Treated HTN
0.04
Framingham Risk Calculation Coefficient
Baseline Risk of CV Event, Male Smoker with Treated HTN
0.23
Framingham Risk Calculation Coefficient
Multiplier for Probability of MI from CV Risk
0.22
Landi 2018
87
D’Agostino 2008
88
Schultz 2021
89
Multiplier for Probability of Stroke from CV Risk
0.23
Multiplier for Probability of Other CV Disease from CV Risk
0.55
Risk Equations
Onset of Cardiovascular Condition, 10-Year Risk: Office-Based Non-Laboratory Pred. Model
Baseline and Beta Coefficient
Women
Men
So(10)
0.94833
0.8843
Log of Age
2.72107
3.113
BMI
0.51125
0.7928
Log of SBP if Not Treated
2.81291
1.8551
Log of SBP if Treated
2.88267
1.9267
Smoking
0.61868
0.7095
Diabetes
0.77763
0.5316
Framingham Risk Calculation Coefficient
88
Onset of Diabetes, Annual Risk: 1.46×10
-6
exp (1.87×HbA1C) × 1.97×10
-2
exp (0.101×BMI)
Exponential regression from Edelman et al.
85
Comorbidity Annual Cost Inputs
Cost Other CV Disease
$14,279
Scully 2017
97
Cost Acute Stroke
$17,316
HCUP
98
Cost Post Stroke
$6,500
Kazi 2019
99
Cost Acute MI
$26,034
HCUP
98
Cost Post MI
$3,117
Kazi 2016
100
Cost, First Year
$27,030
Patel 2021
101
; Urbich 2020
102
Cost HF, Second Year or Later
$15,605
Patel 2021
101
Cost DM
$11,425
ADA 2018
103
Quality of Life Inputs
Utility with Normal BMI†
0.9442-
0.0007×Age
Sullivan 2006
104
Disutility per BMI Unit Increase
-0.0033
Kim 2022
105
; Pi-Sunyer 2015
43
Multiplicative Utility – Other CV Disease
0.959
Sullivan 2006
104
Disutility – Acute Stroke‡
-0.190
Matza 2015
Multiplicative Utility – Post-Stroke
0.943
Sullivan 2006
104
Disutility – Acute MI‡
-0.150
Matza 2015
Multiplicative Utility – Post-MI
0.955
Sullivan 2006
104
Multiplicative Utility – HF
0.930
Multiplicative Utility – DM
0.962
BMI: body mass index, B/N: bupropion/naltrexone, CV: cardiovascular, DM: diabetes mellitus, HbA1C: glycated hemoglobin, HF: heart failure, HTN:
hypertension, ICER: Institute for Clinical and Economic Review, LIR: liraglutide, LSM: lifestyle modification, NMA: network meta-analysis, P/T:
phentermine/topiramate, SBP: systolic blood pressure, SEM: semaglutide
*This cardiovascular model does not include inputs of anti-obesity medication changes in blood pressure, lipids, sleep apnea, cancer, and physical
inactivity (e.g., immobility or osteoarthritis).
†Midpoint of the normal BMI range of 18.5-25 kg/m
2
.
‡Disutility for a 30-day acute condition management.

©Institute for Clinical and Economic Review, 2022 Page 48
Evidence Report – Medications for Obesity Management Return to Table of Contents
Starting utility was derived from age-specific utility values for patients with the characteristics of
the target population.
104
A utility gain was applied for each unit of weight loss due to treatment.
The linear association between weight gain and utility loss was extracted from a recent cost-
effectiveness analysis and trial data.
43,105
For comorbidities associated with higher BMI, we used consistent health state utility values across
all evaluated treatments. Health state disutilities due to cardiovascular comorbid conditions,
diabetes mellitus, and heart failure were derived from systematic literature reviews, utility-specific
patient preference research articles cited in prior cost-effectiveness assessments, and
manufacturer-submitted data. A multiplicative approach was used to apply the health utility value
changes for each of the Markov states. To address the significant decrease in the health utility for
acute event management, we applied daily disutilities for acute myocardial infarction and acute
stroke management for 30 days, an anticipated duration influenced by the significant loss of
mobility and self-care. Subcutaneous injections of GLP-1 receptor agonists are expected to have a
small impact on the overall health state utility compared to the impact of chronic conditions. Thus,
we did not include a utility decrease for the subcutaneous administration of semaglutide or
liraglutide.
For estimates of net pricing, drug costs, and discounts, data are available from both the SSR Health
pricing database and US Department of Veterans Affairs Federal Supply Schedule Service (FSS)
database. Since SSR discount/rebate data were not available for semaglutide for weight loss,
phentermine/topiramate for the most recent quarter, and bupropion/naltrexone for the most
recent quarter, we opted to use the net price from the US FSS database.
Table 4.3. Drug Costs
Drug
List Price
Rebates/
Discounts from
WAC
Model Inputs from FSS Data
Year One
Annual WAC
Year 2+ Annual
WAC
Year One
Annual Net
Year 2+ Annual
Net
Semaglutide
$17,597
$17,597
22.6%*
$13,618
$13,618
Liraglutide
$15,795
$16,424
28.4%†
$11,309
$11,760
Phentermine/
Topiramate
$2,382 $2,429 39.7-57.8%* $1,355 $1,465
Bupropion/
Naltrexone
$7,393 $7,612 72.5%* $2,034 $2,095
FSS: Federal Supply Schedule, WAC: wholesale acquisition cost
*Rebates taken from FSS due to no available net price evidence in SSR Health for the most recent year.
†Rebates taken from SSR Health.
Standard lifestyle modification, consisting of diet and physical activity recommendations, was a
background health care intervention across all treatment arms of the model. The cost of lifestyle
modification was identified by review of prior economic outcome assessment studies.

©Institute for Clinical and Economic Review, 2022 Page 49
Evidence Report – Medications for Obesity Management Return to Table of Contents
Cost of care for cardiovascular comorbid conditions was identified from targeted literature reviews.
The acute care costs of myocardial infarction and stroke were identified from a Healthcare Cost and
Utilization Project National Inpatient Sample database online query. Long-term care costs for post-
myocardial infarction, post-stroke, other cardiovascular disease, heart failure, and diabetes mellitus
were identified from review of prior economic outcome assessments.
Productivity costs, such as those due to patient absenteeism or presenteeism, and caregiver costs
were identified from a review of prior economic assessments and were used to calculate the
indirect costs of the cardiovascular conditions in question under the modified societal
perspective.
103,106-108
4.3. Results
Base-Case Results
The discounted total life years gained, QALYs gained, evLYs gained, and total costs over the lifetime
horizon are shown for each of the obesity treatment strategies in Table 4.4. Incremental values
compared to lifestyle modification are presented in Table 4.5. Undiscounted base-case results are
presented in Supplement E.
Table 4.4. Discounted Base-Case Results
Treatment
Drug Cost
Non-Drug Cost
Total Cost
Life Years
QALYs
evLYs
Semaglutide
$285,800
$106,200
$392,100
21.04
17.85
17.86
Liraglutide
$241,800
$135,200
$377,000
20.86
17.36
17.37
Phentermine/Topiramate
$39,700
$142,800
$182,600
20.85
17.40
17.41
Bupropion/Naltrexone
$52,200
$155,100
$207,300
20.78
17.18
17.19
Lifestyle Modification*
$11,400
$167,800
$179,200
20.70
16.95
16.95
evLY: equal-value life year, QALY: quality-adjusted life year
*Reference for evLY calculation for all active treatments.
Table 4.5. Select Discounted Incremental Results for the Base Case
Incremental Values vs. Lifestyle Modification
Treatment
Drug Cost
Non-Drug Cost
Total Cost
Life Years
QALYs
evLYs
Semaglutide
$274,400
- $61,600
$212,900
0.34
0.90
0.91
Liraglutide
$230,400
- $32,600
$197,800
0.16
0.41
0.42
Phentermine/Topiramate
$28,300
- $25,000
$3,400
0.16
0.45
0.46
Bupropion/Naltrexone
$40,800
-$12,700
$28,100
0.08
0.23
0.23
Lifestyle Modification*
--
--
--
--
--
--
evLY: equal-value life year, QALY: quality-adjusted life year
*Reference for incremental calculation for all active treatments.

©Institute for Clinical and Economic Review, 2022 Page 50
Evidence Report – Medications for Obesity Management Return to Table of Contents
Incremental cost per QALY, life year gained, and evLY gained over the lifetime horizon are shown in
Table 4.6 for each of the obesity treatment strategies.
Table 4.6. Incremental Cost-Effectiveness Ratios for the Base Case
Treatment Comparator
Cost per Life
Year Gained
Cost per QALY
Gained
Cost per
evLY Gained
Semaglutide
Lifestyle modification
$624,000
$238,000
$235,000
Liraglutide
Lifestyle modification
$1,210,000
$485,000
$475,000
Phentermine/Topiramate
Lifestyle modification
$22,000
$8,000
$7,000
Bupropion/Naltrexone
Lifestyle modification
$359,000
$124,000
$121,000
Semaglutide
Liraglutide
$85,000
$31,000
$30,800
Phentermine/topiramate
$1,128,000
$472,000
$468,000
Bupropion/naltrexone
$703,000
$277,000
$274,000
evLY: equal-value life year, QALY: quality-adjusted life year
Sensitivity Analyses
The model was sensitive to several inputs, including the disutility per BMI change, effectiveness of
each treatment in weight loss, baseline HbA1C, and cost of diabetes mellitus. Disutility per BMI
change was most important for semaglutide and liraglutide. The cost of diabetes mellitus
management was most impactful for phentermine/topiramate. Varying the weight-lowering effect
of each treatment compared to lifestyle management and varying the baseline HbA1C had a
considerable influence across all four treatment options. The full one-way sensitivity analysis
results are shown in the Supplement
. Probabilistic sensitivity analysis results in are shown in Table
4.7.
Table 4.7. Results of Probabilistic Sensitivity Analysis by Cost per QALY Gained
Treatment Comparator
Cost
Effective at
$50,000
per QALY
Gained
Cost
Effective at
$100,000
per QALY
Gained
Cost
Effective at
$150,000
per QALY
Gained
Cost
Effective at
$200,000
per QALY
Gained
Semaglutide
Lifestyle modification
0.0%
0.0%
1.0%
8.7%
Liraglutide
Lifestyle modification
0.0%
0.0%
0.0%
0.0%
Phentermine/Topiramate
Lifestyle modification
67.4%
87.0%
92.5%
94.9%
Bupropion/Naltrexone
Lifestyle modification
1.1%
12.4%
38.4%
59.0%
Semaglutide
Phentermine/topiramate
0.0%
0.0%
0.0%
0.0%
Bupropion/naltrexone
0.0%
0.0%
0.0%
2.0%
QALY: quality-adjusted life year

©Institute for Clinical and Economic Review, 2022 Page 51
Evidence Report – Medications for Obesity Management Return to Table of Contents
Scenario Analyses
Conducting the analysis from a societal perspective had some impact on estimates of cost
effectiveness (see Tables 4.8 and 4.9 and Supplement Tables E11 and E12
). Having the same
proportion of men and women (50:50) in the model or changing baseline BMI in scenario analyses
had a modest impact on the estimates (see Supplement Tables
E16-E18). Table 4.10 presents
scenarios with use of an additional Drug X (scenario with effect on weight loss seen in the SUPPORT
1 trial of tirzepatide and pricing of semaglutide for overweight and obesity and effects on blood
pressure and diabetes mellitus similar to semaglutide), use of generic phentermine/topiramate, and
use of generic bupropion/naltrexone. The incremental cost-effectiveness ratio for the lifetime
weight management with Drug X versus lifestyle modification was $145,300 per QALY gained at the
annual Drug X cost of $13,618. The lifetime drug cost for generic phentermine/topiramate was
$14,000 (compared to $39,700 for branded therapy in the base case) and for generic
bupropion/naltrexone was $25,500 (compared to $52,200 for branded therapy in the base case).
Two scenario analyses evaluating the potential impact of cancer or chronic kidney disease (i.e.,
Comorbidity X scenario analyses) had modest impacts on the cost effectiveness of most
medications for obesity management (see Supplement Tables
E13-E15).
Table 4.8. Discounted Results from the Societal Perspective
Treatment Drug Cost
Non-Drug
Cost
Total Cost
Life
Years
QALYs evLYs
Semaglutide
$285,800
$145,300
$431,200
21.04
17.85
17.86
Liraglutide
$241,800
$183,500
$425,200
20.86
17.36
17.37
Phentermine/Topiramate
$39,700
$193,100
$232,800
20.85
17.40
17.41
Bupropion/Naltrexone
$52,200
$209,200
$261,400
20.78
17.18
17.19
Lifestyle Modification*
$11,400
$226,000
$237,400
20.70
16.95
16.95
evLY: equal-value life year, QALY: quality-adjusted life year
*Reference for evLY calculation for all active treatments.

©Institute for Clinical and Economic Review, 2022 Page 52
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 4.9. Discounted Incremental Results from the Societal Perspective
Incremental Values vs. Lifestyle Modification
Treatment Drug Cost
Non-Drug
Cost
Total
Cost
Life Years QALYs evLYs
Semaglutide
$274,400
-$80,700
$193,800
0.34
0.90
0.91
Liraglutide
$230,400
-$42,500
$187,800
0.16
0.41
0.42
Phentermine/Topiramate
$28,300
-$32,900
-$4,600
0.15
0.45
0.46
Bupropion/Naltrexone
$40,800
-$16,755
$24,058
0.08
0.23
0.23
Lifestyle Modification*
--
--
--
--
--
--
Incremental Cost Effectiveness Ratio vs. Lifestyle Modification
Cost/Life
Year Gained
Cost/QALY
Gained
Cost/evLY
Gained
Semaglutide
$568,300
$216,600
$213,900
Liraglutide
$1,149,200
$460,900
$451,400
Phentermine/Topiramate
Less costly, more effective
Bupropion/Naltrexone
$307,000
$106,000
$104,000
evLY: equal-value life year, QALY: quality-adjusted life year
*Reference for incremental calculation for all active treatments.
Table 4.10. Scenario Analysis Results (Drug X and Generic Combination)
Treatment Drug Cost
Non-Drug
Cost
Total Cost Life Years QALYs evLYs
Drug X
$283,600
$83,500
$367,100
21.18
18.25
18.26
Generic P/T
$14,000
$142,800
$156,800
20.85
17.40
17.41
Generic B/N
$25,500
$155,100
$180,600
20.78
17.18
17.19
LSM
$11,400
$167,800
$179,200
20.70
16.95
16.95
Incremental Value vs. LSM
Drug X
$272,200
-$84,300
$188,000
0.48
1.30
1.31
Generic P/T
$2,600
-$24,900
-$22,400
0.15
0.45
0.46
Generic B/N
$14,100
-$12,700
$1,400
0.08
0.23
0.23
Incremental Cost-Effectiveness (QALY) Ratio
vs. Lifestyle Management
Cost/Life Year
Gained
Cost/QALY
Gained
Cost/evLY
Gained
Drug X
$387,400
$145,300
$144,400
Generic P/T
Generic P/T less costly, more effective
Generic B/N
$18,000
$6,000
$6,000
B/N: bupropion/naltrexone, evLY: equal-value life year, LSM: lifestyle modification, LY: life year, P/T:
phentermine/topiramate, QALY: quality-adjusted life year
Note: Drug X is assumed to achieve 17.8% BMI reduction with 0.44 decrease in HbA1C with an overall
discontinuation rate of 6.5%.

©Institute for Clinical and Economic Review, 2022 Page 53
Evidence Report – Medications for Obesity Management Return to Table of Contents
Threshold Analyses
The annualized prices required to achieve thresholds of $50,000 to $200,000 per QALY and evLY
gained are presented in Tables 4.11 and 4.12.
Table 4.11. QALY-Based Threshold Analysis Results
Annual
Net Price
Annualized
Price to
Achieve
$50,000 per
QALY Gained
Annualized
Price to
Achieve
$100,000 per
QALY Gained
Annualized
Price to
Achieve
$150,000 per
QALY Gained
Annualized
Price to
Achieve
$200,000 per
QALY Gained
Semaglutide
$13,618
$5,275
$7,494
$9,714
$11,933
Liraglutide
$11,760
$2,714
$3,753
$4,791
$5,830
Phentermine/Topiramate
$1,465
$2,440
$3,591
$4,741
$5,892
Bupropion/Naltrexone
$2,094
$1,241
$1,823
$2,396
$2,980
Lifestyle Modification
Reference
QALY: quality-adjusted life year
Table 4.12. evLY-Based Threshold Analysis Results
Annual
Net Price
Annualized
Price to
Achieve
$50,000 per
evLY Gained
Annualized
Price to
Achieve
$100,000 per
evLY Gained
Annualized
Price to
Achieve
$150,000 per
evLY Gained
Annualized
Price to
Achieve
$200,000 per
evLY Gained
Semaglutide
$13,618
$5,298
$7,547
$9,793
$12,048
Liraglutide
$11,760
$2,725
$3,791
$4,851
$5,912
Phentermine/Topiramate
$1,465
$2,471
$3,656
$4,840
$6,021
Bupropion/Naltrexone
$2,094
$1,252
$1,844
$2,434
$3,025
Lifestyle Modification
Reference
evLY: equal-value life year
Model Validation
Model validation followed standard practices in the field. All mathematical functions in the model
were tested to assess face validity and to ensure consistency with the Report. We also conducted
sensitivity analyses with null input values to ensure the model was producing findings consistent
with expectations. Further, the model was subjected to internal and external review to evaluate
the mathematical functions as well as the specific inputs and corresponding outputs.
Model validation was also conducted in terms of comparisons to other model findings. We
searched the literature to identify models that were similar to our analysis, with comparable
populations, settings, perspective, and treatments. We also identified a publication that evaluated
semaglutide and other drugs for medication-assisted treatment of weight loss.
105
This recently
published model differed from ours in structure and inputs, including having additional Markov
states and differences in the handling of multiple comorbidities, a two-year treatment period

©Institute for Clinical and Economic Review, 2022 Page 54
Evidence Report – Medications for Obesity Management Return to Table of Contents
instead of lifetime, a 30-year time horizon instead of lifetime, handling excess mortality due to
obesity in a different manner, using a higher cost of semaglutide, and having different utility inputs.
When we changed our model inputs to resemble theirs (i.e., higher semaglutide unit cost, utility
inputs, two-year treatment, and 30-year time horizon), our incremental cost-effectiveness estimate
comparing semaglutide to lifestyle modification ($115,500) approached their reported estimate
comparing semaglutide to diet and exercise ($122,549). The remaining difference in these
incremental cost-effectiveness estimates could likely be explained by a much shorter 30-year life
expectancy in all treatments reported in their model.
Finally, a targeted literature search was conducted to review mortality and cardiovascular events
from real-world evidence and to compare the real-world data with those predicted by the model.
The average remaining life expectancy of a 45-year-old US female is 38.08 years.
109
In one study,
class I obesity shortened life expectancy by approximately 3.5 years in middle-aged women.
110
Our
model estimate was comparable to this real-world data, with an expected remaining median
survival of 34 years and a predominantly female population taking semaglutide. Our model
produced estimates for the cumulative incidence of cardiovascular conditions of 59.5% in patients
receiving lifestyle management. The cumulative estimated incidence in patients receiving
semaglutide was 52.1%. These model findings reflect the lifetime cardiovascular risk estimates
from real-world studies in patients with an average age of 45 years living with major risk factors or
obesity.
111,112
Supplement E7
contains additional information about model validation results.
Uncertainty and Controversies
In 2013, the American Medical Association recognized obesity as a chronic disease.
113
As a result,
long-term weight management includes both weight loss and maintenance of weight reduction.
However, medications for weight management are often not covered or require a stepped
approach to care, with access granted only after lifestyle changes and other treatments have
failed.
114
Where medications are covered, restrictions may be imposed on the duration of
treatment (e.g., through day supply/quantity limits or reauthorization criteria). The Government
Accountability Office showed that, between 2008 and 2017, 78.4% of first treatment episodes users
had a medication duration of 91 days or less.
114
In contrast, after discussions with several experts in
our scoping discussions, most stated that lifetime treatment with medications is now the preferred
approach to managing obesity and overweight, given weight regain after discontinuation and the
need for long-term use to prevent comorbid disease and mortality. As a result of this input, we
decided to evaluate lifetime treatment as the base-case analysis.
Another important uncertainty in the model was that the medications used for weight management
often had multiple effects on the body in addition to weight loss. To limit the complexity of the
cost-effectiveness model and to prevent double-counting of treatment benefits, we limited the

©Institute for Clinical and Economic Review, 2022 Page 55
Evidence Report – Medications for Obesity Management Return to Table of Contents
long-term effects of treatments for weight management to cardiovascular risk and delays in the
onset and/or diagnosis of diabetes mellitus (in patients starting in the model without diabetes) due
to the effect of medications on A1C. As a result, there may be additional benefits with certain
therapies that were not captured in the model. For example, GLP-1 receptor agonists have been
shown to improve cardiovascular risk to a greater extent than expected by changes to HbA1C and
weight loss alone in patients with diabetes mellitus.
29,43
These effects of GLP-1 receptor agonists
have not yet been well elucidated in patients without diabetes mellitus, the starting population
within the base-case model.
The long-term benefits of preventing other comorbidities including cancer, chronic kidney disease,
osteoarthritis, and sleep apnea were not explicitly modeled in the base case. Though obesity is
associated with cancer risk, a clear causal relationship has not been established between weight
loss and the extent to which cancer-specific outcomes change. The short-term quality of life gains
from decreased pain from osteoarthritis and improved sleep were included as general
improvements in health-related utility associated with changes in BMI. With regard to chronic
kidney disease, the costs and disutility of chronic kidney disease secondary to diabetes mellitus and
heart failure were implicitly captured in the model. The impact of treatment on chronic kidney
disease risk arising from overweight and obesity, independent of the effects on diabetes mellitus
and heart failure, could not be quantified and was not included in the base case. Similarly, the
cardiovascular benefits of reduced sleep apnea were already implicitly included in the equation
used to estimate cardiovascular risk. However, the potential cost savings arising from a reduced
need for osteoarthritis or sleep apnea treatments with substantial weight loss were believed to be
small relative to the costs of cardiovascular conditions and diabetes mellitus and were not included
in the base-case simulation. To further explore the potential impact of comorbid conditions
partially included or excluded from the base-case analysis, we tested the potential impact of weight
loss on cancer risk and chronic kidney disease using add-on Comorbidity X Markov states. These
scenario analyses did not significantly alter the incremental cost-effectiveness ratios, alleviating
concerns about the effects of these comorbidities on the cost effectiveness of weight management
strategies.
Bupropion is an approved treatment for smoking cessation, which may also improve cardiovascular
risk. Additionally, smoking cessation can lead to weight gain.
115
Since we wanted to evaluate the
impact of these treatments on weight loss alone, the potential benefits of bupropion for patients
wanting to quit smoking were not included in the model.
The key drivers of cost effectiveness in our model were health state utility, effectiveness of
medication in reducing weight, and factors associated with prevention of diabetes mellitus, such as
reduction in HbA1C with treatment and baseline HbA1C. Cardiovascular benefits of GLP-1 receptor
agonists that appear to extend beyond their impact on weight loss and HbA1C improvements have
been shown in patients with diabetes mellitus. Although not evaluated in our model, additional

©Institute for Clinical and Economic Review, 2022 Page 56
Evidence Report – Medications for Obesity Management Return to Table of Contents
cardiovascular benefits, if present for GLP-1 receptor agonists in patients without diabetes mellitus,
could result in improved cost effectiveness of treatment with semaglutide and liraglutide.
There are several important limitations in this analysis. As described above, we did not include the
full potential impact of weight loss on chronic kidney disease and other conditions for which weight
loss may be beneficial, such as preventing a number of cancers. Some conditions (e.g., sleep apnea,
chronic kidney disease) were purposely excluded due to a concern over double-counting the
beneficial effects of weight loss. Other conditions (e.g., cancer) were excluded due to insufficient
evidence documenting the impact of weight loss on reductions in those conditions or their related
costs.
The equations used in our model were developed to determine the associations among patient-
related factors, including weight and first cardiovascular events. These equations may have
limitations when attempting to predict the impact of medication-assisted treatment for weight loss,
especially in the case of medications that have complex actions on the body.
Because the analysis
was limited by available evidence, the outcomes of preventing or treating obesity in subpopulations
with larger potential benefits (e.g., younger individuals, women of childbearing age, or underserved
populations) were not specifically addressed.
4.4. Summary and Comment
We conducted an analysis of the cost effectiveness of medication-assisted therapy for weight loss,
administered over an individual’s lifetime, using a Markov health state transition model. All
therapies added to lifestyle modification conferred health gains as compared to lifestyle
modification alone in accordance with their incremental weight loss and corresponding
cardiovascular and metabolic benefits. Revised results suggest that at current estimates of net
price, neither semaglutide nor liraglutide were cost effective given commonly accepted thresholds.
In contrast, phentermine/topiramate in addition to lifestyle modification was cost effective per
commonly accepted thresholds owing to its comparatively smaller net acquisition costs.
Bupropion/naltrexone was cost effective at higher thresholds only and would require discounted
prices to meet lower thresholds.
When the treatments were compared to each other, phentermine/topiramate plus lifestyle
modification was less costly and more effective than bupropion/naltrexone plus lifestyle
modification. However, for patients not achieving desired weight loss or unable to tolerate
phentermine/topiramate, bupropion/naltrexone may be a cost-effective alternative. Semaglutide
(plus lifestyle modification) was more effective and more costly than both phentermine/topiramate
and bupropion/naltrexone but did not meet commonly accepted cost-effectiveness thresholds for
either comparison. As such, semaglutide may be considered in patients not achieving desired
weight loss or unable to tolerate phentermine/topiramate or bupropion/naltrexone, but only with a
significant discount.

©Institute for Clinical and Economic Review, 2022 Page 57
Evidence Report – Medications for Obesity Management Return to Table of Contents
5. Contextual Considerations and Potential
Other Benefits
Our reviews seek to provide information on potential other benefits offered by the intervention to
the individual patient, caregivers, the delivery system, other patients, or the public that was not
available in the evidence base nor could be adequately estimated within the cost-effectiveness
model. These elements are listed in the table below, with related information gathered from
patients and other stakeholders. Following the public deliberation on this report the appraisal
committee will vote on the degree to which each of these factors should affect overall judgments of
long-term value for money of the intervention(s) in this review.
Table 5.1. Contextual Considerations
Contextual Consideration
Relevant Information
Acuity of need for treatment of individual
patients based on short-term risk of death
or progression to permanent disability
Not applicable
Magnitude of the lifetime impact on
individual patients of the condition being
treated
Obesity is a chronic disease that usually begins early in life and can
continue throughout the course of a patient’s life broadly affecting
physical, psychosocial, and emotional health. As such, it can affect
educational achievement, workplace opportunities and
performance assessments, and personal relationship.
There is uncertainty about how short-term
mild to moderate weight loss translates into
long-term benefits in preventing obesity-
related disease morbidity and mortality
Though evidence from trials of semaglutide, liraglutide,
phentermine/topiramate, and bupropion/naltrexone in patients
with obesity showed sustained weight loss and few serious side
effects over short-term follow-up, the long-term benefits of the
chronic use of these medications remains uncertain. This relates to
the ability to maintain use over long periods given evidence for
weight regain upon discontinuation, the benefits of mild to
moderate weight loss on clinical outcomes, and potential
differences in the medications underlying mechanisms that may be
associated with other beneficial or harmful aspects on clinical
outcomes beyond any sustained weight loss.

©Institute for Clinical and Economic Review, 2022 Page 58
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table 5.2. Potential Other Benefits or Disadvantages
Potential Other Benefit or Disadvantage
Relevant Information
Patients’ ability to achieve major life goals
related to education, work, or family life
New medications for obesity that lead to sustained weight loss and
improve the symptoms and complications of obesity may help
improve quality of life across a range of different outcomes
including social interactions with family, friends and other relations,
educational achievement, and work opportunities and
performance. This is particularly true for women of childbearing age
where the potential effect of weight reduction on fertility, maternal
morbidity and mortality, and infant health may be improved with
weight loss. However, it is uncertain whether semaglutide,
liraglutide, phentermine/topiramate, and/or bupropion/naltrexone
will improve these outcomes.
Caregivers’ quality of life and/or ability to
achieve major life goals related to
education, work, or family life
Though children and adolescents with obesity often require care
involving family members and other caregivers, this Report focused
on adults with obesity. Even among adults with obesity, its impact
may fall not only on the patient, but also on caregivers. As such,
new medications that promote sustained weight loss offer the
possibility of improving the quality of life for caregivers as well as
for patients.
Patients’ ability to manage and sustain
treatment given the complexity of regimen
Use of phentermine/topiramate and bupropion/naltrexone, which
are oral therapies and do not require the daily or weekly injections,
may decrease the complexity of care. All four medications may be
less complex to use on a long-term basis than constant attention to
diet and physical activity.
Society’s goal of reducing health inequities
Obesity disproportionally impacts certain racial and ethnic groups,
and emphasizes the need for and potential impact of improved
treatment options. However, the costs of medications for obesity
are often not covered by health insurance, and there are
differences among individuals in their ability to access health care.
This may exacerbate existing health inequities by selectively limiting
access of these medications to those patients who are able to
afford them and have access to health care providers who can
prescribe them.
Additionally, ICER calculated the Health Improvement Distribution
Index, looking at the relative proportion of any health gains from
treatment of overweight with one or more comorbidities and
obesity for the following groups who have a higher prevalence of
overweight with comorbidities and obesity than the general US
population.
116
• African American/Black female: 1.3
•
Hispanic: 1.1
These medications offer new mechanisms of
action that may allow more patients to
achieve meaningful weight loss among those
who have failed other treatments or may
wish to avoid surgical therapies
Semaglutide and liraglutide, GLP-1 receptor agonists, represent
medications that reflect research in which improved understanding
of the mechanisms of disease have led to new therapies.

©Institute for Clinical and Economic Review, 2022 Page 59
Evidence Report – Medications for Obesity Management Return to Table of Contents
6. Health-Benefit Price Benchmarks
Health-benefit price benchmarks for the annual cost of treatment with the semaglutide are
presented in Table 6.1. The health-benefit price benchmark for a drug is defined as the price range
that would achieve incremental cost-effectiveness ratios between $100,000 and $150,000 per QALY
or evLY gained. Based on our model analyses, we estimate a health-benefit price benchmark range
for semaglutide from $7,500 to $9,800 per QALY or evLY gained compared to lifestyle modification
alone. Corresponding discounts from WAC to achieve the health-benefit price benchmark range for
semaglutide compared to lifestyle modification alone range from 44-57%.
Table 6.1. Annual Cost-Effectiveness Health-Benefit Price Benchmarks for Semaglutide plus
Lifestyle Modification vs. Lifestyle Modification Alone plus Background Therapy
Outcome for
Annual Health-
Benefit Price
Benchmark
Calculation
Annual WAC
Annual Price at
$100,000 Threshold
Annual Price at
$150,000 Threshold
Discount from WAC
to Reach Threshold
Prices
Semaglutide plus Lifestyle Modification vs. Lifestyle Modification Alone
QALYs Gained
$17,597.48
$7,500
$9,700
45-57%
evLYs Gained
$17,597.48
$7,600
$9,800
44-57%
evLY: equal-value life year, QALY: quality-adjusted life-year, WAC: wholesale acquisition cost

©Institute for Clinical and Economic Review, 2022 Page 60
Evidence Report – Medications for Obesity Management Return to Table of Contents
7. Potential Budget Impact
7.1. Overview of Key Assumptions
Using results from the cost-effectiveness model, we estimated the potential budget impact of
adding semaglutide to current lifestyle modification for US adults with BMI ≥30 or 27.0
kg/m
2
≤BMI<30 kg/m
2
with one or more weight-related comorbidities. In accordance with the
Reference Case
, semaglutide is treated as an intervention in the budget impact analysis, as it has
been on the market for less than two years as of posting the Model Analysis Plan. In contrast,
liraglutide, phentermine/topiramate, and bupropion/naltrexone are treated as comparators, as
they have been on the market for two years or more.
For potential budget impact analyses, we used semaglutide’s list price and net price and three
threshold prices (at $50,000, $100,000, and $150,000 per QALY) compared to lifestyle modification
alone. These additional analyses on semaglutide threshold prices were conducted to inform
budgetary impact estimations aligned with notions of semaglutide’s cost effectiveness as calculated
within the cost-effectiveness analyses. Potential budget impact is defined as the total differential
cost of using semaglutide rather than the relevant existing therapies for the treated population,
calculated as intervention costs minus any offsets in these costs from averted health care events or
other resource utilization. All costs were undiscounted and estimated over a five-year time horizon.
To estimate the size of the potential candidate populations for treatment, we used the US adult
population and prevalence of overweight and obesity given specific weight-related comorbidities or
biomarkers as reported within National Health and Nutrition Examination Survey datasets over the
2017-2018 and 2019-March 2020 data collection cycles.
117
Accordingly, we estimated a combined
prevalence value for US adults with BMI ≥30 kg/m
2
(41.96%) or 27.0 kg/m
2
≤BMI<30 kg/m
2
with one
or more weight-related comorbidities (11.57%) at 53.53%. To quantify the number of these
patients eligible for semaglutide therapy, we identified two cohorts: those currently on medication
treatment for weight management and those seeking medication treatment for weight
management. Accordingly, we estimated that 1.3% of all US adults in the prevalent cohort receive
medication, with another 1.3% seeking medication therapy but not currently receiving it. These
estimates were derived from electronic health record data on 2.2 million adults eligible for weight
loss medication from eight geographically dispersed health care systems across the US, and from
manufacturer data submissions, respectively.
118,119
Applied to the projected US adult population
over 2022-2026, we estimated 3,700,000 adults would be eligible for treatment with semaglutide.
For this analysis, we assumed that 20% of these patients would initiate treatment with semaglutide
in each of the five years (~740,000 per year), for a total of 100% of the cohort being treated with
semaglutide at the end of five years.
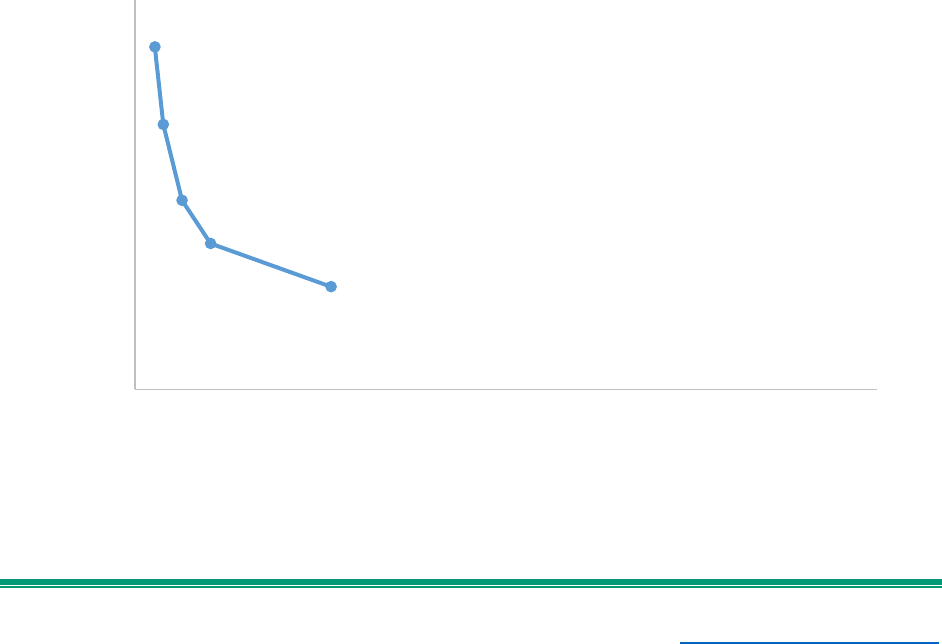
©Institute for Clinical and Economic Review, 2022 Page 61
Evidence Report – Medications for Obesity Management Return to Table of Contents
Of the 1.3% of individuals on medication therapy at baseline, 53%, 30%, and 17% are assigned to
liraglutide, phentermine/topiramate, and bupropion/naltrexone, respectively.
119
The remaining
individuals seeking medication therapy are assigned to lifestyle modification alone at baseline. In
our potential budget impact analyses, semaglutide draws market share proportionally from each of
the model comparators over the five-year time horizon.
7.2. Results
At semaglutide’s estimated net price of $13,618.22 per year, 3.77% of eligible patients could be
treated within five years (assuming 20% uptake each year) without crossing the ICER potential
budget impact threshold of $777 million per year. In contrast, 2.65%, 6.30%, 10.18%, and 26.41% of
eligible patients could be treated within five years without crossing the ICER potential budget
impact threshold at the annual price to reach list price ($17,597.48), $150,000 per QALY ($9,700),
$100,000 per QALY ($7,500), and $50,000 per QALY ($5,300), respectively. The modest percentages
were primarily driven by the large population eligible for treatment with semaglutide. Figure 7.1.
depicts the potential budgetary impact of semaglutide at the annual list price, net price, and three
threshold prices compared to lifestyle modification alone.
Figure 7.1. Budgetary Impact of Semaglutide in US Adults Seeking or Using Medication Therapy
for Weight Management with BMI ≥30 or 27.0 kg/m
2
≤BMI<30 kg/m
2
with One or More Weight-
Related Comorbidities
BI: budget impact, QALY: quality-adjusted life year, WAC: wholesale acquisition cost
Annual WAC
Annual Net Price
$50,000/QALY Annual Price
$100,000/QALY Annual Price
$150,000/QALY Annual Price
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
$16,000
$18,000
$20,000
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Annual Semaglutide Price
Percentage of Patients Treated Without Crossing Potential BI Threshold Each Year

©Institute for Clinical and Economic Review, 2022 Page 62
Evidence Report – Medications for Obesity Management Return to Table of Contents
References
1. Kastanias P, Mackenzie K, Robinson S, Wang W. Medical Complications Resulting from Severe
Obesity. In: Sockalingam S, Hawa R, eds. Psychiatric Care in Severe Obesity. Springer, Cham;
2016:pp. 49-73.
2. Centers for Disease Control and Prevention. About Overweight & Obesity.
https://www.cdc.gov/obesity/about-obesity/index.html
. Published 2021. Accessed March 29,
2022.
3. Crockett KB, Borgatti A, Tan F, Tang Z, Dutton G. Weight Discrimination Experienced Prior to
Enrolling in a Behavioral Obesity Intervention is Associated with Treatment Response Among
Black and White Adults in the Southeastern U.S. Int J Behav Med. 2021.
4. Arterburn DE, Olsen MK, Smith VA, et al. Association between bariatric surgery and long-term
survival. Jama. 2015;313(1):62-70.
5. Wharton S, Lau DCW, Vallis M, et al. Obesity in adults: a clinical practice guideline. Cmaj.
2020;192(31):E875-e891.
6. Centers for Disease Control and Prevention. Summary Health Statistics: National Health
Interview Survey. Table A-15. Published 2015. Accessed February 28, 2022.
7. Ward ZJ, Bleich SN, Cradock AL, et al. Projected U.S. State-Level Prevalence of Adult Obesity and
Severe Obesity. N Engl J Med. 2019;381(25):2440-2450.
8. Liu B, Du Y, Wu Y, Snetselaar LG, Wallace RB, Bao W. Trends in obesity and adiposity measures
by race or ethnicity among adults in the United States 2011-18: population based study. Bmj.
2021;372:n365.
9. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of Obesity Among Adults and Youth:
United States, 2015-2016. NCHS Data Brief. 2017(288):1-8.
10. Ogden CL. Disparities in obesity prevalence in the United States: black women at risk. Am J Clin
Nutr. 2009;89(4):1001-1002.
11. Cawley J, Biener A, Meyerhoefer C, et al. Direct medical costs of obesity in the United States and
the most populous states. J Manag Care Spec Pharm. 2021;27(3):354-366.
12. Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of
Obesity. N Engl J Med. 2022.
13. Cardel MI, Newsome FA, Pearl RL, et al. Patient-Centered Care for Obesity: How Health Care
Providers Can Treat Obesity While Actively Addressing Weight Stigma and Eating Disorder Risk. J
Acad Nutr Diet. 2022.
14. World Health Organization. Fact Sheet: Obesity and Overweight. WHO. Published 2021.
Accessed February 21, 2022.
15. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of Obesity and Severe Obesity Among
Adults: United States, 2017-2018. NCHS Data Brief. 2020(360):1-8.
16. Moyer VA. Screening for and management of obesity in adults: U.S. Preventive Services Task
Force recommendation statement. Ann Intern Med. 2012;157(5):373-378.
17. Trogdon JG, Finkelstein EA, Hylands T, Dellea PS, Kamal-Bahl SJ. Indirect costs of obesity: a
review of the current literature. Obes Rev. 2008;9(5):489-500.
18. Dor A, Ferguson C, Langwith C, Tan E. A Heavy Burden: The Individual Costs of Being Overweight
and Obese in the United States. The George Washington University, School of Public Health and
Health Services; September 21, 2010 2010.
19. Heymsfield SB, Wadden TA. Mechanisms, Pathophysiology, and Management of Obesity. N Engl
J Med. 2017;376(15):1492.

©Institute for Clinical and Economic Review, 2022 Page 63
Evidence Report – Medications for Obesity Management Return to Table of Contents
20. Cypess AM. Reassessing Human Adipose Tissue. N Engl J Med. 2022;386(8):768-779.
21. Bray GA, Frühbeck G, Ryan DH, Wilding JP. Management of obesity. Lancet.
2016;387(10031):1947-1956.
22. Vallis M. Quality of life and psychological well-being in obesity management: improving the odds
of success by managing distress. Int J Clin Pract. 2016;70(3):196-205.
23. Garvey WT, Mechanick JI, Brett EM, et al. AMERICAN ASSOCIATION OF CLINICAL
ENDOCRINOLOGISTS AND AMERICAN COLLEGE OF ENDOCRINOLOGY COMPREHENSIVE CLINICAL
PRACTICE GUIDELINES FOR MEDICAL CARE OF PATIENTS WITH OBESITY. Endocr Pract. 2016;22
Suppl 3:1-203.
24. Madigan CD, Graham HE, Sturgiss E, et al. Effectiveness of weight management interventions for
adults delivered in primary care: systematic review and meta-analysis of randomised controlled
trials. Bmj. 2022;377:e069719.
25. Curry SJ, Krist AH, Owens DK, et al. Behavioral Weight Loss Interventions to Prevent Obesity-
Related Morbidity and Mortality in Adults: US Preventive Services Task Force Recommendation
Statement. Jama. 2018;320(11):1163-1171.
26. Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and Risks of Bariatric Surgery in
Adults: A Review. Jama. 2020;324(9):879-887.
27. Aminian A, Wilson R, Al-Kurd A, et al. Association of Bariatric Surgery With Cancer Risk and
Mortality in Adults With Obesity. Jama. 2022;327(24):2423-2433.
28. Afshin A, Forouzanfar MH, Reitsma MB, et al. Health Effects of Overweight and Obesity in 195
Countries over 25 Years. N Engl J Med. 2017;377(1):13-27.
29. Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with
Overweight or Obesity. New England Journal of Medicine. 2021;384(11):989-1002.
30. Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with
overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-
dummy, placebo-controlled, phase 3 trial. The Lancet. 2021;397(10278):971-984.
31. Wadden TA, Bailey TS, Billings LK, et al. Effect of Subcutaneous Semaglutide vs Placebo as an
Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity:
The STEP 3 Randomized Clinical Trial. Jama. 2021;325(14):1403-1413.
32. Garvey W, Bhatta M, Davies M, et al. Treatment with Semaglutide 2.4 mg Leads to
Improvements in Cardiometabolic Risk Factors in the STEP 1 Trial. Paper presented at: Obesity
Facts2021.
33. Rubino DM, Greenway FL, Khalid U, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily
Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8
Randomized Clinical Trial. Jama. 2022;327(2):138-150.
34. Clinicaltrials.gov. STEP 1: Research Study Investigating How Well Semaglutide Works in People
Suffering From Overweight or Obesity. In:2020.
35. Clinicaltrials.gov. Research Study to Look at How Well Semaglutide is at Lowering Weight When
Taken Together With an Intensive Lifestyle Program. In:2020.
36. Kushner RF, Calanna S, Davies M, et al. Semaglutide 2.4 mg for the Treatment of Obesity: Key
Elements of the STEP Trials 1 to 5. Obesity (Silver Spring). 2020;28(6):1050-1061.
37. Clinicaltrials.gov. Two-year Research Study Investigating How Well Semaglutide Works in People
Suffering From Overweight or Obesity. In:2021.
38. Garvey WT. Two-year Effect of Semaglutide 2.4 mg vs Placebo in Adults with Overweight or
Obesity: STEP 5. Paper presented at: 39th Annual Meeting of The Obesity Society (TOS)2021;
ObesityWeek.

©Institute for Clinical and Economic Review, 2022 Page 64
Evidence Report – Medications for Obesity Management Return to Table of Contents
39. Perreault L, Davies M, Frias JP, et al. Changes in Glucose Metabolism and Glycemic Status With
Once-Weekly Subcutaneous Semaglutide 2.4 mg Among Participants With Prediabetes in the
STEP Program. Diabetes Care. 2022.
40. Wadden TA, Hollander P, Klein S, et al. Weight maintenance and additional weight loss with
liraglutide after low-calorie-diet-induced weight loss: the SCALE Maintenance randomized study.
Int J Obes (Lond). 2013;37(11):1443-1451.
41. Blackman A, Foster GD, Zammit G, et al. Effect of liraglutide 3.0 mg in individuals with obesity
and moderate or severe obstructive sleep apnea: the SCALE Sleep Apnea randomized clinical
trial. Int J Obes (Lond). 2016;40(8):1310-1319.
42. Davies MJ, Bergenstal R, Bode B, et al. Efficacy of Liraglutide for Weight Loss Among Patients
With Type 2 Diabetes: The SCALE Diabetes Randomized Clinical Trial. Jama. 2015;314(7):687-
699.
43. Pi-Sunyer X, Astrup A, Fujioka K, et al. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in
Weight Management. New England Journal of Medicine. 2015;373(1):11-22.
44. Wadden TA, Tronieri JS, Sugimoto D, et al. Liraglutide 3.0 mg and Intensive Behavioral Therapy
(IBT) for Obesity in Primary Care: The SCALE IBT Randomized Controlled Trial. Obesity (Silver
Spring). 2020;28(3):529-536.
45. Garvey WT, Birkenfeld AL, Dicker D, et al. Efficacy and Safety of Liraglutide 3.0 mg in Individuals
With Overweight or Obesity and Type 2 Diabetes Treated With Basal Insulin: The SCALE Insulin
Randomized Controlled Trial. Diabetes Care. 2020;43(5):1085-1093.
46. Food and Drug Administration. Saxenda (liraglutide) Package Insert - June 2022.
https://www.novo-pi.com/saxenda.pdf
. Published 2022. Accessed.
47. Food and Drug Adminstration. Wegovy (Semaglutide) Package Insert - June 2021.
https://www.novo-pi.com/wegovy.pdf
. Published 2021. Accessed.
48. Clinicaltrials.gov. Effect of Liraglutide on Body Weight in Non-diabetic Obese Subjects or
Overweight Subjects With Co-morbidities: SCALE™ - Obesity and Pre-diabetes. In:2013.
49. Clinicaltrials.gov. Comparison of Liraglutide Versus Placebo in Weight Loss Maintenance in
Obese Subjects: SCALE - Maintenance. In:2010.
50. Clinicaltrials.gov. Effect of Liraglutide in Obese Subjects With Moderate or Severe Obstructive
Sleep Apnoea: SCALE™ - Sleep Apnoea. In:2013.
51. Clinicaltrials.gov. Effect and Safety of Liraglutide 3.0 mg as an Adjunct to Intensive Behaviour
Therapy for Obesity in a Non-specialist Setting. In:2018.
52. Clinicaltrials.gov. Effect of Liraglutide on Body Weight in Overweight or Obese Subjects With
Type 2 Diabetes: SCALE™ - Diabetes. In:2013.
53. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus
topiramate combination on weight and associated comorbidities in overweight and obese adults
(CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377(9774):1341-
1352.
54. Aronne LJ, Wadden TA, Peterson C, Winslow D, Odeh S, Gadde KM. Evaluation of phentermine
and topiramate versus phentermine/topiramate extended-release in obese adults. Obesity.
2013;21(11):2163-2171.
55. Clinicaltrials.gov. A Study Comparing Multiple Doses of VI-0521 With Placebo and Their Single-
agent Constituents for Treatment of Obesity in Adults. In:2008.
56. Allison DB, Gadde KM, Garvey WT, et al. Controlled-release phentermine/topiramate in severely
obese adults: a randomized controlled trial (EQUIP). Obesity (Silver Spring). 2012;20(2):330-342.
57. Clinicaltrials.gov. Study of VI-0521 Compared to Placebo in Treatment of Obesity in Adults.
In:2009.

©Institute for Clinical and Economic Review, 2022 Page 65
Evidence Report – Medications for Obesity Management Return to Table of Contents
58. Garvey WT, Ryan DH, Bohannon NJ, et al. Weight-loss therapy in type 2 diabetes: effects of
phentermine and topiramate extended release. Diabetes Care. 2014;37(12):3309-3316.
59. Hollander P, Gupta AK, Plodkowski R, et al. Effects of naltrexone sustained-release/bupropion
sustained-release combination therapy on body weight and glycemic parameters in overweight
and obese patients with type 2 diabetes. Diabetes Care. 2013;36(12):4022-4029.
60. Clinicaltrials.gov. A Safety and Efficacy Study Comparing Naltrexone SR/Bupropion SR and
Placebo in Obese Subjects With Type 2 Diabetes. In:2009.
61. Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss
in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-
controlled, phase 3 trial. Lancet. 2010;376(9741):595-605.
62. Clinicaltrials.gov. A Study of the Safety and Efficacy of Two Doses of Naltrexone SR/Bupropion SR
and Placebo in Overweight and Obese Subjects. In:2009.
63. Apovian CM, Aronne L, Rubino D, et al. A randomized, phase 3 trial of naltrexone SR/bupropion
SR on weight and obesity-related risk factors (COR-II). Obesity (Silver Spring). 2013;21(5):935-
943.
64. Clinicaltrials.gov. A Safety and Efficacy Study of Naltrexone SR/Bupropion SR in Overweight and
Obese Subjects. In:2009.
65. Wadden TA, Foreyt JP, Foster GD, et al. Weight loss with naltrexone SR/bupropion SR
combination therapy as an adjunct to behavior modification: the COR-BMOD trial. Obesity (Silver
Spring). 2011;19(1):110-120.
66. Clinicaltrials.gov. A Safety and Efficacy Study of Naltrexone SR/Bupropion SR and Placebo in
Overweight and Obese Subjects Participating in an Intensive Behavior Modification Program.
In:2008.
67. Novo Nordisk. Novo Nordisk Data Submission. Data on File. In:2022.
68. Wharton S, Calanna S, Davies M, et al. Gastrointestinal tolerability of once-weekly semaglutide
2.4 mg in adults with overweight or obesity, and the relationship between gastrointestinal
adverse events and weight loss. Diabetes Obes Metab. 2022;24(1):94-105.
69. Kushner RF, Garvey WT, Hesse D, et al. Once-weekly Subcutaneous Semaglutide 2.4 mg Reduces
Body Weight in Adults with Overweight or Obesity Regardless of Baseline Characteristics (STEP
1). Endocrine Society. 2021.
70. Lingvay I, FÆRch L, Koroleva A, et al. 83-OR: Influence of Baseline Characteristics on Weight Loss
with Semaglutide 2.4 mg in Adults with Overweight/Obesity and Type 2 Diabetes (STEP 2).
Diabetes. 2021;70:83-OR.
71. Yoo DH, Prodanovic N, Jaworski J, et al. Efficacy and safety of CT-P13 (biosimilar infliximab) in
patients with rheumatoid arthritis: Comparison between switching from reference infliximab to
CT-P13 and continuing CT-P13 in the PLANETRA extension study. Annals of the rheumatic
diseases. 2016.
72. Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after
withdrawal of semaglutide: The STEP 1 trial extension. Diabetes, Obesity and Metabolism.
2022;24(8):1553-1564.
73. Ryan DH, Lingvay I, Colhoun HM, et al. Semaglutide Effects on Cardiovascular Outcomes in
People With Overweight or Obesity (SELECT) rationale and design. Am Heart J. 2020;229:61-69.
74. Ard J, Cannon A, Lewis CE, et al. Efficacy and safety of liraglutide 3.0 mg for weight management
are similar across races: subgroup analysis across the SCALE and phase II randomized trials.
Diabetes Obes Metab. 2016;18(4):430-435.

©Institute for Clinical and Economic Review, 2022 Page 66
Evidence Report – Medications for Obesity Management Return to Table of Contents
75. King WC, Hinerman AS, Belle SH, Wahed AS, Courcoulas AP. Comparison of the Performance of
Common Measures of Weight Regain After Bariatric Surgery for Association With Clinical
Outcomes. Jama. 2018;320(15):1560-1569.
76. Sheahan KH, Wahlberg EA, Gilbert MP. An overview of GLP-1 agonists and recent cardiovascular
outcomes trials. Postgrad Med J. 2020;96(1133):156-161.
77. Ebong IA, Goff DC, Rodriguez CJ, Chen H, Bertoni AG. Mechanisms of heart failure in obesity.
Obesity Research & Clinical Practice. 2014;8(6):e540-e548.
78. Goff DC, Jr., Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of
cardiovascular risk: a report of the American College of Cardiology/American Heart Association
Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S49-73.
79. Tancredi M, Rosengren A, Svensson AM, et al. Excess Mortality among Persons with Type 2
Diabetes. N Engl J Med. 2015;373(18):1720-1732.
80. Pande RL, Perlstein TS, Beckman JA, Creager MA. Secondary prevention and mortality in
peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004.
Circulation. 2011;124(1):17-23.
81. Odegaard KM, Hallen J, Lirhus SS, Melberg HO, Halvorsen S. Incidence, prevalence, and mortality
of heart failure: a nationwide registry study from 2013 to 2016. ESC Heart Fail. 2020;7(4):1917-
1926.
82. Majed B, Montaye M, Wagner A, et al. All-Cause Mortality up to and After Coronary Heart
Disease and Stroke Events in European Middle-Aged Men: The PRIME Study. Stroke.
2015;46(5):1371-1373.
83. Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with
Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002.
84. Pi-Sunyer X, Astrup A, Fujioka K, et al. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in
Weight Management. N Engl J Med. 2015;373(1):11-22.
85. Edelman D, Olsen MK, Dudley TK, Harris AC, Oddone EZ. Utility of hemoglobin in predicting
diabetes risk. J Gen Intern Med. 2004;19(12):1175-1180.
86. Jakobsen GS, Skottheim IB, Sandbu R, et al. Long-term effects of gastric bypass and duodenal
switch on systemic exposure of atorvastatin. Surg Endosc. 2013;27(6):2094-2101.
87. Landi F, Calvani R, Picca A, et al. Body Mass Index is Strongly Associated with Hypertension:
Results from the Longevity Check-up 7+ Study. Nutrients. 2018;10(12).
88. D'Agostino RB, Sr., Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in
primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753.
89. Schultz BG, Tilton J, Jun J, Scott-Horton T, Quach D, Touchette DR. Cost-Effectiveness Analysis of
a Pharmacist-Led Medication Therapy Management Program: Hypertension Management. Value
in health : the journal of the International Society for Pharmacoeconomics and Outcomes
Research. 2021;24(4):522-529.
90. Borisenko O, Lukyanov V, Debergh I, Dillemans B. Cost-effectiveness analysis of bariatric surgery
for morbid obesity in Belgium. J Med Econ. 2018;21(4):365-373.
91. Borisenko O, Mann O, Dupree A. Cost-utility analysis of bariatric surgery compared with
conventional medical management in Germany: a decision analytic modeling. BMC Surg.
2017;17(1):87.
92. Lopes S, Meincke HH, Lamotte M, Olivieri AV, Lean MEJ. A novel decision model to predict the
impact of weight management interventions: The Core Obesity Model. Obes Sci Pract.
2021;7(3):269-280.

©Institute for Clinical and Economic Review, 2022 Page 67
Evidence Report – Medications for Obesity Management Return to Table of Contents
93. Picot J, Jones J, Colquitt JL, et al. The clinical effectiveness and cost-effectiveness of bariatric
(weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol
Assess. 2009;13(41):1-190, 215-357, iii-iv.
94. Sulo G, Igland J, Vollset SE, et al. Heart Failure Complicating Acute Myocardial Infarction; Burden
and Timing of Occurrence: A Nation-wide Analysis Including 86 771 Patients From the
Cardiovascular Disease in Norway (CVDNOR) Project. J Am Heart Assoc. 2016;5(1).
95. Shi Q, Wang Y, Hao Q, et al. Pharmacotherapy for adults with overweight and obesity: a
systematic review and network meta-analysis of randomised controlled trials. Lancet.
2022;399(10321):259-269.
96. Human Mortality Database. 2022. https://usa.mortality.org/national.php?national=USA
.
Accessed June 1, 2022.
97. Scully RE, Arnaoutakis DJ, DeBord Smith A, Semel M, Nguyen LL. Estimated annual health care
expenditures in individuals with peripheral arterial disease. J Vasc Surg. 2018;67(2):558-567.
98. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project.
https://www.hcup-us.ahrq.gov/databases.jsp
. Published 2022. Accessed June 1, 2022, 2021.
99. Kazi DS, Penko J, Coxson PG, Guzman D, Wei PC, Bibbins-Domingo K. Cost-Effectiveness of
Alirocumab: A Just-in-Time Analysis Based on the ODYSSEY Outcomes Trial. Ann Intern Med.
2019;170(4):221-229.
100. Kazi DS, Moran AE, Coxson PG, et al. Cost-effectiveness of PCSK9 Inhibitor Therapy in Patients
With Heterozygous Familial Hypercholesterolemia or Atherosclerotic Cardiovascular Disease.
Jama. 2016;316(7):743-753.
101. Patel J. Heart failure population health considerations. Am J Manag Care. 2021;27(9
Suppl):S191-S195.
102. Urbich M, Globe G, Pantiri K, et al. A Systematic Review of Medical Costs Associated with Heart
Failure in the USA (2014-2020). Pharmacoeconomics. 2020;38(11):1219-1236.
103. American Diabetes A. Economic Costs of Diabetes in the U.S. in 2017. Diabetes Care.
2018;41(5):917-928.
104. Sullivan PW, Ghushchyan V. Preference-Based EQ-5D index scores for chronic conditions in the
United States. Med Decis Making. 2006;26(4):410-420.
105. Kim N, Wang J, Burudpakdee C, et al. Cost-effectiveness analysis of semaglutide 2.4 mg for the
treatment of adult patients with overweight and obesity in the United States. Journal of
Managed Care & Specialty Pharmacy. 2022;28(7):740-752.
106. Girotra T, Lekoubou A, Bishu KG, Ovbiagele B. A contemporary and comprehensive analysis of
the costs of stroke in the United States. J Neurol Sci. 2020;410:116643.
107. Page RL, 2nd, Ghushchyan V, Gifford B, et al. The economic burden of acute coronary syndromes
for employees and their dependents: medical and productivity costs. J Occup Environ Med.
2013;55(7):761-767.
108. Cook C, Cole G, Asaria P, Jabbour R, Francis DP. The annual global economic burden of heart
failure. Int J Cardiol. 2014;171(3):368-376.
109. Administration SS. Actuarial Life Table. 2022 Trustees Report. 2022.
110. Bhaskaran K, dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall
and cause-specific mortality: a population-based cohort study of 3·6 million adults in the
UK. The Lancet Diabetes & Endocrinology. 2018;6(12):944-953.
111. Wilkins JT, Ning H, Berry J, Zhao L, Dyer AR, Lloyd-Jones DM. Lifetime Risk and Years Lived Free
of Total Cardiovascular Disease. Jama. 2012;308(17):1795-1801.
112. Khan SS, Ning H, Wilkins JT, et al. Association of Body Mass Index With Lifetime Risk of
Cardiovascular Disease and Compression of Morbidity. JAMA Cardiology. 2018;3(4):280-287.

©Institute for Clinical and Economic Review, 2022 Page 68
Evidence Report – Medications for Obesity Management Return to Table of Contents
113. Kyle TK, Dhurandhar EJ, Allison DB. Regarding Obesity as a Disease: Evolving Policies and Their
Implications. Endocrinol Metab Clin North Am. 2016;45(3):511-520.
114. Government Accountability Office. Obesity Drugs. Few adults used prescription drugs for weight
loss and insurance coverage varied. United States Government Accountability Office Report to
Congressional Committees. 2019.
115. Bush T, Lovejoy JC, Deprey M, Carpenter KM. The effect of tobacco cessation on weight gain,
obesity, and diabetes risk. Obesity (Silver Spring). 2016;24(9):1834-1841.
116. (CMS) CfMaMS. National Health and Nutrition Examination Survey (NHANES),. 2021.
117. Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey,
NHANES 2017 - March 2020. 2021.
118. Saxon DR, Iwamoto SJ, Mettenbrink CJ, et al. Antiobesity Medication Use in 2.2 Million Adults
Across Eight Large Health Care Organizations: 2009-2015. Obesity (Silver Spring).
2019;27(12):1975-1981.
119. A/S NN.
120. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019.
Diabetes Care. 2019;42(Suppl 1):S13-s28.
121. Kolotkin RL, Head S, Hamilton M, Tse CK. Assessing Impact of Weight on Quality of Life. Obes
Res. 1995;3(1):49-56.
122. Kolotkin RL, Crosby RD, Kosloski KD, Williams GR. Development of a brief measure to assess
quality of life in obesity. Obes Res. 2001;9(2):102-111.
123. Kolotkin RL, Ervin CM, Meincke HH, Højbjerre L, Fehnel SE. Development of a clinical trials
version of the Impact of Weight on Quality of Life-Lite questionnaire (IWQOL-Lite Clinical Trials
Version): results from two qualitative studies. Clin Obes. 2017;7(5):290-299.
124. Kolotkin RL, Williams VSL, Ervin CM, et al. Validation of a new measure of quality of life in
obesity trials: Impact of Weight on Quality of Life-Lite Clinical Trials Version. Clin Obes.
2019;9(3):e12310.
125. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual
framework and item selection. Medical care. 1992;30(6):473-483.
126. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J
Gen Intern Med. 2001;16(9):606-613.
127. Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH. The Inventory of Depressive
Symptomatology (IDS): psychometric properties. Psychol Med. 1996;26(3):477-486.
128. Mayer SB, Graybill S, Raffa SD, et al. Synopsis of the 2020 U.S. VA/DoD Clinical Practice Guideline
for the Management of Adult Overweight and Obesity. Mil Med. 2021;186(9-10):884-896.
129. Apovian CM, Aronne LJ, Bessesen DH, et al. Pharmacological management of obesity: an
endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2015;100(2):342-362.
130. Stegenga H, Haines A, Jones K, Wilding J. Identification, assessment, and management of
overweight and obesity: summary of updated NICE guidance. Bmj. 2014;349:g6608.
131. Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: synthesis of best evidence for clinical
decisions. Ann Intern Med. 1997;126(5):376-380.
132. Higgins J, Thomas, J, Chandler, J, Cumpston, M, Li, T, Page, MJ, Welch, VA. Cochrane Handbook
for Systematic Reviews of Interventions version 6.1 (updated September 2020).
https://training.cochrane.org/handbook/current
. Published 2020. Accessed.
133. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for
reporting systematic reviews. BMJ. 2021;372:n71.
134. Agency for Healthcare Research and Quality. U.S. Preventive Services Task Force Procedure
Manual. Published 2008. Accessed.

©Institute for Clinical and Economic Review, 2022 Page 69
Evidence Report – Medications for Obesity Management Return to Table of Contents
135. Ollendorf DA, Pearson SD. An integrated evidence rating to frame comparative effectiveness
assessments for decision makers. Medical care. 2010;48(6 Suppl):S145-152.
136. Ollendorf D, Pearson, SD. ICER Evidence Rating Matrix: A User's Guide.
https://icer-
review.org/methodology/icers-methods/icer-evidence-ratingmatrix/. . Published 2020. Updated
January 31, 2020. Accessed.
137. Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons.
Stat Med. 2004;23(20):3105-3124.
138. Caldwell DM, Ades AE, Higgins JP. Simultaneous comparison of multiple treatments: combining
direct and indirect evidence. BMJ. 2005;331(7521):897-900.
139. Dias S, Welton NJ, Caldwell DM, Ades AE. Checking consistency in mixed treatment comparison
meta-analysis. Stat Med. 2010;29(7-8):932-944.
140. Rubino D, Abrahamsson N, Davies M, et al. Effect of Continued Weekly Subcutaneous
Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The
STEP 4 Randomized Clinical Trial. Jama. 2021;325(14):1414-1425.
141. Clinicaltrials.gov. Research Study Investigating How Well Semaglutide Works in People Suffering
From Overweight or Obesity. In:2020.
142. Kadowaki T, Isendahl J, Khalid U, et al. Semaglutide once a week in adults with overweight or
obesity, with or without type 2 diabetes in an east Asian population (STEP 6): a randomised,
double-blind, double-dummy, placebo-controlled, phase 3a trial. The Lancet Diabetes &
Endocrinology. 2022;10(3):193-206.
143. Gudbergsen H, Overgaard A, Henriksen M, et al. Liraglutide after diet-induced weight loss for
pain and weight control in knee osteoarthritis: a randomized controlled trial. Am J Clin Nutr.
2021;113(2):314-323.
144. Winslow DH, Bowden CH, DiDonato KP, McCullough PA. A Randomized, Double-Blind, Placebo-
Controlled Study of an Oral, Extended-Release Formulation of Phentermine/Topiramate for the
Treatment of Obstructive Sleep Apnea in Obese Adults. Sleep. 2012;35(11):1529-1539.
145. Nissen SE, Wolski KE, Prcela L, et al. Effect of Naltrexone-Bupropion on Major Adverse
Cardiovascular Events in Overweight and Obese Patients With Cardiovascular Risk Factors: A
Randomized Clinical Trial. Jama. 2016;315(10):990-1004.
146. Clinicaltrials.gov. Cardiovascular Outcomes Study of Naltrexone SR/Bupropion SR in Overweight
and Obese Subjects With Cardiovascular Risk Factors (The Light Study). In:2015.
147. Halseth A, Shan K, Walsh B, Gilder K, Fujioka K. Method-of-use study of naltrexone sustained
release (SR)/bupropion SR on body weight in individuals with obesity. Obesity (Silver Spring).
2017;25(2):338-345.
148. Clinicaltrials.gov. A Study of VI-0521 for the Treatment of Obstructive Sleep Apnea Hypopnea
Syndrome in Obese Adults. In:2009.
149. Clinicaltrials.gov. Method-of-Use Study Assessing the Effect of Naltrexone Sustained Release
(SR)/ Bupropion SR on Body Weight and Cardiovascular Risk Factors in Overweight and Obese
Subjects. In:2014.
150. Arastu N, Cummins O, Uribe W, Nemec EC. Efficacy of subcutaneous semaglutide compared to
placebo for weight loss in obese, non-diabetic adults: a systematic review & meta-analysis. Int J
Clin Pharm. 2022.
151. Sanders GD, Neumann PJ, Basu A, et al. Recommendations for Conduct, Methodological
Practices, and Reporting of Cost-effectiveness Analyses: Second Panel on Cost-Effectiveness in
Health and Medicine. Jama. 2016;316(10):1093-1103.
152. Jiang R, Janssen MFB, Pickard AS. US population norms for the EQ-5D-5L and comparison of
norms from face-to-face and online samples. Quality of Life Research. 2021;30(3):803-816.

©Institute for Clinical and Economic Review, 2022 Page 70
Evidence Report – Medications for Obesity Management Return to Table of Contents
153. US Department of Health & Human Services. Current Cigarette Smoking Among Adults in the
United States. In: Centers for Diasese Control and Prevention, ed. Atlanta, GA. 2022.
154. Organisation for Economic Co-operation and Development. OECD.Stat. https://stats.oecd.org/
.
Published 2022. Accessed July 11, 2022.
155. Peters SAE, Colantonio LD, Dai Y, et al. Trends in Recurrent Coronary Heart Disease After
Myocardial Infarction Among US Women and Men Between 2008 and 2017. Circulation.
2021;143(7):650-660.
156. Kolmos M, Christoffersen L, Kruuse C. Recurrent Ischemic Stroke - A Systematic Review and
Meta-Analysis. J Stroke Cerebrovasc Dis. 2021;30(8):105935.
157. Wang Y, Wang QJ. The prevalence of prehypertension and hypertension among US adults
according to the new joint national committee guidelines: new challenges of the old problem.
Arch Intern Med. 2004;164(19):2126-2134.
158. American Heart Association American Stroke Association. Cardiovascular disease: A costly
burden for America. Projections through 2035.
https://www.heart.org/-/media/files/get-
involved/advocacy/burden-report-consumer-report.pdf. Published 2017. Accessed August 19,
2022.
159. White MC, Holman DM, Boehm JE, Peipins LA, Grossman M, Henley SJ. Age and cancer risk: a
potentially modifiable relationship. Am J Prev Med. 2014;46(3 Suppl 1):S7-15.
160. Munsell MF, Sprague BL, Berry DA, Chisholm G, Trentham-Dietz A. Body mass index and breast
cancer risk according to postmenopausal estrogen-progestin use and hormone receptor status.
Epidemiol Rev. 2014;36:114-136.
161. Mohammedi K, Chalmers J, Herrington W, et al. Associations between body mass index and the
risk of renal events in patients with type 2 diabetes. Nutr Diabetes. 2018;8(1):7.
162. United States Renal Data System. USRDS Annual Data Report | Volume 1 - CKD in the United
States. Chapter 3: Morbidity and Mortality in Patients with CKD. 2015.
https://www.usrds.org/media/1549/vol1_03_morbidity_mortality_15.pdf
. Published 2015.
Accessed July 11, 2022.
163. United States Renal Data System. 2021 USRDS Annual Data Report: Epidemiology of kidney
disease in the United States. National Institutes of Health, National Institute of Diabetes and
Digestive and Kidney Diseases, Bethesda, MD, 2021. https://adr.usrds.org/2021
. Published 2021.
Accessed.
164. Borisenko O, Adam D, Funch-Jensen P, et al. Bariatric Surgery can Lead to Net Cost Savings to
Health Care Systems: Results from a Comprehensive European Decision Analytic Model. Obes
Surg. 2015;25(9):1559-1568.
165. Borisenko O, Lukyanov V, Ahmed AR. Cost-utility analysis of bariatric surgery. Br J Surg.
2018;105(10):1328-1337.
166. Borisenko O, Lukyanov V, Johnsen SP, Funch-Jensen P. Cost analysis of bariatric surgery in
Denmark made with a decision-analytic model. Dan Med J. 2017;64(8).
167. Lopes S, Johansen P, Lamotte M, McEwan P, Olivieri AV, Foos V. External Validation of the Core
Obesity Model to Assess the Cost-Effectiveness of Weight Management Interventions.
Pharmacoeconomics. 2020;38(10):1123-1133.
168. Lee M, Lauren BN, Zhan T, et al. The cost-effectiveness of pharmacotherapy and lifestyle
intervention in the treatment of obesity. Obes Sci Pract. 2020;6(2):162-170.
169. Hu Y, Zheng SL, Ye XL, et al. Cost-effectiveness analysis of 4 GLP-1RAs in the treatment of obesity
in a US setting. Ann Transl Med. 2022;10(3):152.

©Institute for Clinical and Economic Review, 2022 Page 71
Evidence Report – Medications for Obesity Management Return to Table of Contents
170. Thillainadesan S, Madsen S, James DE, Hocking SL. The impact of weight cycling on health
outcomes in animal models: A systematic review and meta-analysis. Obes Rev.
2022;23(5):e13416.
171. Rhee EJ. Weight Cycling and Its Cardiometabolic Impact. J Obes Metab Syndr. 2017;26(4):237-
242.


©Institute for Clinical and Economic Review, 2022 Page A1
Evidence Report – Medications for Obesity Management Return to Table of Contents
A. Background: Supplemental Information
A1. Definitions
Obesity: BMI is the most common way that obesity is defined in clinical practice. Overweight is
considered a BMI of 25 kg/m
2
to 29.9 kg/m
2
. Obesity is considered a BMI of 30 kg/m2 or greater. It
is further subclassified as level I (30 kg/m
2
to 34.9 kg/m
2
), level II (35 kg/m
2
to 39.9 kg/m
2
), or level
III (40 kg/m
2
or more).
Pre-diabetes: The clinical trials assessed patients for pre-diabetes using slightly different criteria.
Pre-diabetes is defined by the American Diabetes Association based on an HbA1C result of 5.7%-
6.4% (39-47 mmol/mol), a fasting glucose of 100-125 mg/dL (5.6-6.9 mmol/L), or a two-hour oral
glucose tolerance test of 140-mg-199 mg/dL (7.8-11.0 mmol/L).
120
Important outcomes in the pivotal trials studied include:
Percentage weight loss: This primary outcome in most studies represents the mean percentage
point change in weight at follow-up relative to the baseline body weight.
Categorical weight loss (≥5%): This is a co-primary outcome in many studies and represents the
percentage of individuals who achieve a ≥5% change in body weight from baseline to follow-up
assessment. Greater weight loss can be assessed using ≥10%, ≥15%, or higher percentages.
Impact of Weight on Quality of Life-Lite Clinical Trials Version (IWQOL-Lite-CT): The IWQOL was
the first quality of life instrument specifically developed to assess individuals with obesity.
121
It
measures those aspects of quality of life that were identified by individuals with moderate or severe
obesity to be of greatest concern. Eight domains assessed include health, social/interpersonal,
work, mobility, self-esteem, sexual life, activities of daily living, and comfort with food. Originally a
74-item instrument, the IWQOL-Lite is a shorter, 31-item, self-reported version that consists of a
total score and scores on each of five scales: Physical Function, Self-Esteem, Sexual Life, Public
Distress, and Work.
122
The IWQOL-Lite Clinical Trials Version (IWQOL-Lite-CT), was developed and
validated for use in clinical trials.
123,124
It is a 20-item measure used to assess weight-related
physical and psychosocial functioning in three composite scores (physical, physical function, and
psychosocial) and a total score. The range of possible scores for the IWQOL-Lite-CT is 0-100. For
the IWQOL-Lite-CT, an increase in score is representative of an improvement in health status.
Short Form-36 v2® Health Survey, Acute Version (SF-36): The SF-36 is a generic quality of life
measure widely used to assess patient-reported functional outcomes.
125
It includes 36 questions
across eight domains (physical functioning, role limitations due to physical health problems, body
pain, general health, vitality, social functioning, role limitations due to emotional problems, and

©Institute for Clinical and Economic Review, 2022 Page A2
Evidence Report – Medications for Obesity Management Return to Table of Contents
mental health). Additionally, the SF-36 domains can be aggregated into two scores, the Physical
Component Summary (PCS) and the Mental Component Summary (MCS). For the SF-36, an increase
in score is representative of an improvement in health status.
Patient Health Questionnaire (PHQ-9): The PHQ-9 is a self-administered instrument to measure
symptoms of depression.
126
It was derived from the PRIME-MD diagnostic instrument for common
mental disorders. Each item asks the individual to rate daily symptoms from "0" (not at all) to "3"
(nearly every day). A higher score indicated worse depressive symptoms.
Inventory of Depressive Symptomatology (Self-Report) (IDS-SR): The IDS-SR is a 30-item
questionnaire measuring depressive symptoms. Each item has four statements that reflect various
degrees of symptom severity, scored on a four-point scale from 0 to 3.
127
A higher score indicated
worse depressive symptoms.
A2. Potential Cost-Saving Measures in Obesity Management
ICER includes in its reports information on wasteful or lower-value services in the same clinical area
that could be reduced or eliminated to create headroom in health care budgets for higher-value
innovative services (for more information, see
https://icer.org/our-approach/methods-
process/value-assessment-framework/). These services are ones that would not be directly
affected by semaglutide, liraglutide, phentermine/topiramate, and/or bupropion/naltrexone (e.g.,
need for obstructive sleep apnea treatment), as these services will be captured in the economic
model. Rather, we are seeking services used in the current management of obesity beyond the
potential offsets that arise from a new intervention. During stakeholder engagement and public
comment periods, ICER encouraged all stakeholders to suggest services (including treatments and
mechanisms of care) currently used for individuals with obesity that could be reduced, eliminated,
or made more efficient. No suggestions were received.
A3. Future Therapies
In June 2022, results from the SURMOUNT-1 trial of tirzepatide were published.
12
Tirzepatide is
both a GLP-1 receptor agonist and also a glucose-dependent insulinotropic polypeptide receptor
agonist. ICER previously reviewed tirzepatide
as a treatment for type 2 diabetes mellitus. The
manufacturer of tirzepatide requested that it not be added to this report as the current ICER
evaluation process was already underway. Tirzepatide is neither an intervention nor a comparator
in this Report. However, to provide context, we review the results of SURMOUNT-1 here.
SURMOUNT-1 was a 72-week Phase III trial comparing three doses of tirzepatide and placebo in
2,539 adults without diabetes and with a BMI ≥30 kg/m
2
,
or ≥27 kg/m
2
with one weight-related
complication. Tirzepatide was administered by weekly subcutaneous injection at doses of 5 mg, 10
mg, or 15 mg, with an initial 20-week dose-escalation period.

©Institute for Clinical and Economic Review, 2022 Page A3
Evidence Report – Medications for Obesity Management Return to Table of Contents
The mean baseline BMI in the study population was 38. Tirzepatide at doses of 5 mg, 10 mg, and 15
mg resulted in greater percentage reductions in weight than placebo (15.0%, 19.5%, and 20.9% vs.
3.1%, respectively). More patients achieved categorical weight reduction targets as well. For
example, a ≥5% target was achieved by 85.1%, 88.9%, and 90.9% of patients, respectively, with the
tirzepatide doses, versus 34.5% with placebo. A ≥25% target was achieved by 15.3%, 32.3%, and
36.2% of patients, respectively, with tirzepatide versus 1.5% with placebo.
Patients treated with tirzepatide also experienced improvements in physical functioning, decreases
in systolic and diastolic blood pressure, improvements in lipids, and decreases in fasting insulin
levels.
Most adverse events with tirzepatide were gastrointestinal in nature and discontinuation for
adverse events occurred in more patients treated with tirzepatide than placebo (4.3%, 7.1%, and
6.2% vs. 2.6%, respectively). Gastrointestinal adverse events were typically worse at initiation or
dose escalation of tirzepatide, with improvement over time.

©Institute for Clinical and Economic Review, 2022 Page B1
Evidence Report – Medications for Obesity Management Return to Table of Contents
B. Patient Perspectives: Supplemental
Information
B1. Methods
In developing and executing this Report, we received valuable input from individual patients and
patient organizations throughout the scoping and evidence development process. We received
public comments on our draft scoping document from the Obesity Action Coalition. We also
conducted a focus group with six patients that was arranged through the Obesity Action Coalition.
These interviews with patients helped to illustrate the diversity of experiences of patients living
with obesity as well as highlighting the health outcomes that were most important to them.

©Institute for Clinical and Economic Review, 2022 Page C1
Evidence Report – Medications for Obesity Management Return to Table of Contents
C. Clinical Guidelines
Veterans’ Health Administration/Department of Defense
Clinical Practice Guideline for the Management of Adult Overweight and Obesity
128
The Evidence-Based Practice Work Group of the Department of Veterans Affairs and the
Department of Defense released updated guideline recommendations in 2020. These
recommendations updated a prior evidence review released in 2014. A number of key elements of
weight loss and management were highlighted. Obesity is recognized as a chronic disease requiring
long-term management. Shared decision-making involving patients and providers is seen as a
fundamental aspect of weight management. Managing obesity involves addressing all of the
factors that may be involved for a given patient. This may include assessing whether medications or
treatments for other conditions may exacerbate weight issues for a patient. Lifestyle interventions
involving comprehensive use of behavioral, dietary, and physical activity components are central to
success in reducing and sustaining weight loss. Pharmacotherapy and weight loss surgery should be
considered along with comprehensive lifestyle interventions, and when instituted they require long-
term follow-up.
In terms of pharmacotherapy, the use of FDA-approved medications needs to consider potential
side effects as well as patient tolerability and preferences. Weight regain can occur with any
medication after discontinuation, so long-term use to maintain weight loss is often needed. Specific
pharmacotherapies that can be offered to patients include bupropion/naltrexone, liraglutide,
orlistat, or phentermine/topiramate. Eligibility includes patients with a BMI ≥30 kg/m
2
and for
those with a BMI ≥27 kg/m
2
who also have obesity-associated conditions. There is insufficient
information to recommend phentermine monotherapy or other stimulants for intermittent, short-
term, or long-term use.
Canadian Clinical Practice Guideline
Obesity in Adults: A Clinical Practice Guideline
5
This guideline was funded by the Canadian Institutes of Health Research Strategic Patient-Oriented
Research initiative, Obesity Canada’s Fund for Obesity Collaboration and Unified initiative, and the
Canadian Association of Bariatric Physicians and Surgeons. An executive and steering committee
with broad expertise and geographic representation was created. The scope of the guideline was
developed by the executive committee. A literature review was performed by the McMaster
Evidence Review and Synthesis Team. Guideline recommendations were formulated by the
steering committee along with chapter leads and authors. Seven individuals living with obesity

©Institute for Clinical and Economic Review, 2022 Page C2
Evidence Report – Medications for Obesity Management Return to Table of Contents
were engaged and one participated on the steering committee. This guideline updated the first
Canadian obesity guideline published in 2006.
Key points emphasized that obesity is a common, complex, progressive, and relapsing disease. It is
characterized by abnormal or excessive body fat that impairs health. Newer insights into appetite
regulation and the underlying mechanisms leading to obesity have opened new approaches for
treating this chronic disease. People living with obesity face substantial bias and stigma, and this
contributes independently of weight or BMI to morbidity and mortality. Reducing weight bias and
stigma, better understanding of the underlying causes of obesity, and supporting patient-centered
care can improve the wellbeing of those living with obesity. Obesity care should be based on
evidence-based principles of chronic disease management, validate patients’ lived experiences, and
move beyond the simplistic notion that obesity requires eating less and increasing activity.
In terms of pharmacotherapy, the guideline focuses on individuals with BMI ≥30 kg/m
2
or BMI ≥27
kg/m
2
with comorbid conditions. Pharmacotherapy is meant to be an adjunctive for weight loss and
weight loss maintenance in addition to medical nutrition therapy, physical activity, and
psychological interventions. Recommended options include liraglutide 3.0 mg,
bupropion/naltrexone, and orlistat. Details of the recommendations are available online in the
chapter titled “Pharmacotherapy in Obesity Management.” Pharmacotherapy is intended to
augment the magnitude of weight loss beyond what can be achieved with health behavior changes
alone. It is also emphasized as being important for the prevention of weight regain.
Endocrine Society
Pharmacological Management of Obesity Guideline
129
This evidence-based guideline was developed by members of the Endocrine Society, the European
Society of Endocrinology, and the Obesity Society. Weight loss is seen as a path to achieving
improved health for patients with obesity-associated risk factors and comorbidities. Medications
approved for chronic weight management can be useful adjuncts to lifestyle interventions for
patients that have not met weight loss goals on their own. Diet, exercise, and behavioral
modification are recommended for patients with BMI ≥25 kg/m
2
and should be included with other
obesity management interventions. Pharmacotherapy can be considered for those with BMI ≥27
kg/m
2
with comorbidity or BMI over 30 kg/m
2
. Patients with a history of being unable to
successfully lose and maintain weight are candidates for weight loss medications. Patients
responding well to weight loss (5% or more after three months) should continue with therapy. In
addition to addressing medications that can promote weight loss, the guidelines emphasize
attention to the use of medications for other conditions that are weight-neutral and avoiding those
that are associated with weight gain.

©Institute for Clinical and Economic Review, 2022 Page C3
Evidence Report – Medications for Obesity Management Return to Table of Contents
Specific pharmacotherapy recommendations include avoiding sympathomimetic agents such as
phentermine in patients with diabetes mellitus and uncontrolled hypertension or a history of heart
disease. In patients with type 2 diabetes mellitus who are overweight or have obesity, antidiabetic
medications that may promote weight loss, such as GLP-1 receptor agonists or sodium-glucose-
linked transporter-2 inhibitors, are suggested. Off-label use of medications approved for other
conditions is not recommended for the sole purpose of weight loss.
National Institute for Health and Care Excellence (NICE)
Obesity: Identification, Assessment, and Management Clinical Guideline
130
NICE released recommendations for managing obesity in 2014. Areas of focus for this guideline
included identification, assessment, and management of obesity. Interventions assessed included
lifestyle, behavioral, physical activity, dietary, pharmacological, and surgical interventions. In terms
of lifestyle interventions, multi-component ones are considered the treatment of choice, and
should include behavioral change strategies that can support increased physical activity and
improved eating habits.
Pharmacological treatment is recommended only after dietary, exercise, and behavioral approaches
have been initiated. One should consider drug treatment of interested individuals who have not
reached their target weight loss. Pharmacological treatments may be continued to maintain weight
loss. For those who have not reached their weight loss target, consideration should be given for
stopping the drug. Since weight loss may be slower in individuals who also have type 2 diabetes
mellitus, less strict goals and longer duration of therapy may be appropriate. Orlistat should only
be prescribed when it is part of an overall plan for managing obesity, should not be co-prescribed
with other weight loss drugs, and should not be continued beyond three months if the person has
not lost at least 5% of their initial body weight. Phentermine/topiramate was not mentioned in this
document, but is listed as being in development.
In December 2017, NICE released recommendations for bupropion/naltrexone. It was not
recommended for managing overweight and obesity in adults alongside a reduced-calorie diet and
increased physical activity. In February, 2022, NICE released a draft guideline for the use of
semaglutide for weight management. It is an option when given in addition to diet and activity
recommendations for individuals with a BMI of at least 35 kg/m
2
or 30-34.9 kg/m
2
with other
comorbid conditions that meet NICE criteria. It can be used for a maximum of two years and needs
to be given by a specialist weight management service. Consideration for stopping semaglutide if
less than 5% initial weight loss has been achieved after six months of maintenance therapy.

©Institute for Clinical and Economic Review, 2022 Page D1
Evidence Report – Medications for Obesity Management Return to Table of Contents
D. Comparative Clinical Effectiveness:
Supplemental Information
D1. Detailed Methods
PICOTS
Population
The population of focus for the review is adults with a BMI ≥30 kg/m
2
or ≥27 kg/m
2
with at least one
weight-related comorbid condition (such as hypertension, type 2 diabetes mellitus, obstructive
sleep apnea, or hyperlipidemia) who are actively seeking medical management for weight loss.
Data permitting, we sought to examine the following patient subgroups, including but not limited
to:
• BMI categories: 27-29.9, 30-34.9, 35-39.9, or greater than 40 kg/m
2
• Pre-diabetes or diabetes mellitus
• Prior bariatric surgery
Interventions
The full list of interventions is as follows:
• Semaglutide
• Liraglutide
• Bupropion and naltrexone in combination
• Phentermine and topiramate in combination
Comparators
We intended to compare each intervention with lifestyle modification to placebo with lifestyle
modification. Data permitting, we also compared the interventions to one another.

©Institute for Clinical and Economic Review, 2022 Page D2
Evidence Report – Medications for Obesity Management Return to Table of Contents
Outcomes
The outcomes of interest are described in the list below.
• Patient-Important Outcomes
o Quality of life and functional status
o Anxiety and depression
o Body image
o Long-term health outcomes such as cardiovascular disease, cancer, and mortality
o Weight loss (as measured by % weight loss, categorical weight loss [e.g., 5%, 10%, or
15%], BMI, etc.)
o Weight re-gain
o Adverse events including:
Side effects
Psychological harm
Serious adverse events
• Other Outcomes
o Metabolic profile, such as LDL, hemoglobin A1C, and blood pressure
o Weight cycling
o Waist circumference
o Progression from pre-diabetes to diabetes mellitus or pre-hypertensive to
hypertensive
o Withdrawal or dose reduction in concomitant medications for weight-related
comorbidities
o Subsequent surgical interventions for weight loss
o Discontinuation due to adverse events
Timing
Evidence on intervention effectiveness was derived from studies of at least 12 weeks duration and
evidence on harms from studies of any duration.
Settings
All relevant settings were considered, with a focus on outpatient settings in the US.

©Institute for Clinical and Economic Review, 2022 Page D3
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D1. PRISMA 2020 Checklist
Section and Topic
Item
#
Checklist item
Reported
on Page #
TITLE
Title
1
Identify the report as a systematic review.
ABSTRACT
Abstract
2
See the PRISMA 2020 for Abstracts checklist.
INTRODUCTION
Rationale 3
Describe the rationale for the review in the context of existing
knowledge.
Objectives 4
Provide an explicit statement of the objective(s) or question(s) the
review addresses.
METHODS
Eligibility Criteria 5
Specify the inclusion and exclusion criteria for the review and how
studies were grouped for the syntheses.
Information
Sources
6
Specify all databases, registers, websites, organizations, reference
lists and other sources searched or consulted to identify studies.
Specify the date when each source was last searched or consulted.
Search Strategy 7
Present the full search strategies for all databases, registers, and
websites, including any filters and limits used.
Selection Process 8
Specify the methods used to decide whether a study met the
inclusion criteria of the review, including how many reviewers
screened each record and each report retrieved, whether they
worked independently, and if applicable, details of automation
tools used in the process.
Data Collection
Process
9
Specify the methods used to collect data from reports, including
how many reviewers collected data from each report, whether
they worked independently, any processes for obtaining or
confirming data from study investigators, and if applicable, details
of automation tools used in the process.
Data Items
10a
List and define all outcomes for which data were sought. Specify
whether all results that were compatible with each outcome
domain in each study were sought (e.g., for all measures, time
points, analyses), and if not, the methods used to decide which
results to collect.
10b
List and define all other variables for which data were sought (e.g.,
participant and intervention characteristics, funding sources).
Describe any assumptions made about any missing or unclear
information.
Study Risk of Bias
Assessment
11
Specify the methods used to assess risk of bias in the included
studies, including details of the tool(s) used, how many reviewers
assessed each study and whether they worked independently, and
if applicable, details of automation tools used in the process.
Effect Measures 12
Specify for each outcome the effect measure(s) (e.g., risk ratio,
mean difference) used in the synthesis or presentation of results.
Synthesis Methods 13a
Describe the processes used to decide which studies were eligible
for each synthesis (e.g., tabulating the study intervention
characteristics and comparing against the planned groups for each
synthesis [item #5]).

©Institute for Clinical and Economic Review, 2022 Page D4
Evidence Report – Medications for Obesity Management Return to Table of Contents
Section and Topic
Item
#
Checklist item
Reported
on Page #
13b
Describe any methods required to prepare the data for
presentation or synthesis, such as handling of missing summary
statistics, or data conversions.
13c
Describe any methods used to tabulate or visually display results of
individual studies and syntheses.
13d
Describe any methods used to synthesize results and provide a
rationale for the choice(s). If meta-analysis was performed,
describe the model(s), method(s) to identify the presence and
extent of statistical heterogeneity, and software package(s) used.
13e
Describe any methods used to explore possible causes of
heterogeneity among study results (e.g. subgroup analysis, meta-
regression).
13f
Describe any sensitivity analyses conducted to assess robustness of
the synthesized results.
Reporting Bias
Assessment
14
Describe any methods used to assess risk of bias due to missing
results in a synthesis (arising from reporting biases).
Certainty
Assessment
15
Describe any methods used to assess certainty (or confidence) in
the body of evidence for an outcome.
RESULTS
Study Selection
16a
Describe the results of the search and selection process, from the
number of records identified in the search to the number of
studies included in the review, ideally using a flow diagram.
16b
Cite studies that might appear to meet the inclusion criteria, but
which were excluded, and explain why they were excluded.
Study
Characteristics
17 Cite each included study and present its characteristics.
Risk of Bias in
Studies
18 Present assessments of risk of bias for each included study.
Results of
Individual Studies
19
For all outcomes, present, for each study: (a) summary statistics
for each group (where appropriate) and (b) an effect estimates and
its precision (e.g., confidence/credible interval), ideally using
structured tables or plots.
Results of
Syntheses
20a
For each synthesis, briefly summarize the characteristics and risk of
bias among contributing studies.
20b
Present results of all statistical syntheses conducted. If meta-
analysis was done, present for each the summary estimate and its
precision (e.g., confidence/credible interval) and measures of
statistical heterogeneity. If comparing groups, describe the
direction of the effect.
20c
Present results of all investigations of possible causes of
heterogeneity among study results.
20d
Present results of all sensitivity analyses conducted to assess the
robustness of the synthesized results.
Reporting Biases 21
Present assessments of risk of bias due to missing results (arising
from reporting biases) for each synthesis assessed.
Certainty of
Evidence
22
Present assessments of certainty (or confidence) in the body of
evidence for each outcome assessed.

©Institute for Clinical and Economic Review, 2022 Page D5
Evidence Report – Medications for Obesity Management Return to Table of Contents
Section and Topic
Item
#
Checklist item
Reported
on Page #
DISCUSSION
Discussion
23a
Provide a general interpretation of the results in the context of
other evidence.
23b
Discuss any limitations of the evidence included in the review.
23c
Discuss any limitations of the review processes used.
23d
Discuss implications of the results for practice, policy, and future
research.
OTHER INFORMATION
Registration and
Protocol
24a
Provide registration information for the review, including register
name and registration number, or state that the review was not
registered.
24b
Indicate where the review protocol can be accessed, or state that a
protocol was not prepared.
24c
Describe and explain any amendments to information provided at
registration or in the protocol.
Support 25
Describe sources of financial or non-financial support for the
review, and the role of the funders or sponsors in the review.
Competing
Interests
26 Declare any competing interests of review authors.
Availability of Data,
Code, and Other
Materials
27
Report which of the following are publicly available and where
they can be found: template data collection forms; data extracted
from included studies; data used for all analyses; analytic code; any
other materials used in the review.
From: Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: An updated guideline for reporting
systematic reviews. PLoS Med. 2021;18(3):e1003583.
Data Sources and Searches
Procedures for the systematic literature review assessing the evidence on treatments for obesity
management followed established best research methods.
131,132
We conducted the review in
accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses
(PRISMA) guidelines.
133
The PRISMA guidelines include a checklist of 27 items.
We searched MEDLINE, EMBASE, Cochrane Database of Systematic Reviews, and Cochrane Central
Register of Controlled Trials for relevant studies. Each search was limited to English-language
studies of human subjects and excluded articles indexed as guidelines, letters, editorials, narrative
reviews, case reports, or news items. We included abstracts from conference proceedings
identified from the systematic literature search. All search strategies were generated utilizing the
Population, Intervention, Comparator, and Study Design elements described above. The proposed
search strategies included a combination of indexing terms (MeSH terms in MEDLINE and EMTREE
terms in EMBASE) as well as free-text terms.
To supplement the database searches, we performed manual checks of the reference lists of
included trials and systematic reviews and invited key stakeholders to share references germane to

©Institute for Clinical and Economic Review, 2022 Page D6
Evidence Report – Medications for Obesity Management Return to Table of Contents
the scope of this project. We also supplemented our review of published studies with data from
conference proceedings, regulatory documents, information submitted by manufacturers, and
other grey literature when the evidence met ICER standards (for more information, see
https://icer.org/policy-on-inclusion-of-grey-literature-in-evidence-reviews/
. Where feasible and
deemed necessary, we also accepted data submitted by manufacturers “in-confidence,” in
accordance with ICER’s published guidelines on acceptance and use of such data
(
https://icer.org/guidelines-on-icers-acceptance-and-use-of-in-confidence-data-from-
manufacturers-of-pharmaceuticals-devices-and-other-health-interventions/).
Table D2. Search Strategy of EMBASE Search
Search Term
#1
‘obesity’/exp OR ‘obesity’
#2
‘body weight loss’/exp OR ‘body weight loss’
#3
(‘obes*’ OR ‘body mass ind*’ OR ‘adiposity’ OR ‘overweight’ OR ‘over weight’ OR ‘anti-obesity’ OR ‘body-
weight’ OR ‘body weight’):ti,ab
#4
#1 OR #2 OR #3
#5
‘phentermine plus topiramate’/exp
#6
((‘phentermine’ AND ‘topiramate’) OR ‘phentermine plus topiramate’ OR ‘qysmia’ OR ‘qsiva’ OR ‘VI-0521’
OR ‘VI0521’ OR ‘VI 0521’):ti,ab
#7
‘amfebutamone plus naltrexone’/exp
#8
(‘amfebutamone plus naltrexone’ OR ‘contrave’ OR (‘amfebutamone’ AND ‘naltrexone’) OR (‘bupropion’
AND ‘naltrexone’) OR ‘CID 11556075’ OR ‘CID11556075’ OR ‘CID-11556075’):ti,ab
#9
‘glucagon like peptide 1 receptor agonist’/exp
#10
‘liraglutide’/exp
#11
(‘liraglutide’ OR ‘saxenda’ OR ‘victoza’ OR ‘NN 2211’ OR ‘NN2211’ OR ‘NN-2211’):ti,ab
#12
‘semaglutide’/exp
#13
(‘semaglutide’ OR ‘ozempic’ OR ‘wegovy’ OR ‘NN 9535’ OR ‘NN9535’ OR ‘NN-9535’):ti,ab
#14
(‘phentermine’ OR ‘Adipex-P’ OR ‘Lomaira’ OR ‘Suprenza’):ti,ab
#15
#5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14
#16
#4 AND #15
#17
#16 NOT ('addresses' OR 'autobiography' OR 'bibliography' OR 'biography' OR 'case report' OR 'comment'
OR 'congresses' OR 'consensus development conference' OR 'duplicate publication' OR 'editorial' OR
'guideline' OR 'in vitro' OR 'interview' OR 'lecture' OR 'legal cases' OR 'legislation' OR 'letter' OR 'news' OR
'newspaper article' OR 'patient education handout' OR 'periodical index' OR 'personal narratives' OR
'portraits' OR 'practice guideline' OR 'review' OR 'video audio media')/it
#18
('animal'/exp OR 'nonhuman'/exp OR 'animal experiment'/exp) NOT 'human'/exp
#19
#17 NOT #18
#20
#19 AND [English]/lim
#21
#20 NOT [medline]/lim
#22
#21 AND [01/07/2020]/sd
*Search last updated on July 18, 2022.

©Institute for Clinical and Economic Review, 2022 Page D7
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D3. Search Strategy of Medline 1996 to Present with Daily Update and Cochrane Central
Register of Controlled Trials
Search Term
1
exp Obesity/
2
exp Weight Loss/
3
exp Overweight/
4
(obes* or "body mass inde*" or adiposity or overweight or "over weight" or antiobesity or "anti-obesity"
or bodyweight or "body weight").ti,ab.
5
1 or 2 or 3 or 4
6
((phentermine and topiramate) or "phentermine topiramate" or phenterminetopiramate or qsymia or
qsiva or topiramatephentermine or "phentermine-topiramate" or VI0521 or "VI 0521" or "VI-0521").ti,ab.
7
((amfebutamone and naltrexone) or (bupropion and naltrexone) or contrave or "bupropion-naltrexone"
or CID11556075 or "CID 11556075" or "CID-11556075").ti,ab.
8
exp Glucagon-Like Peptides/
9
exp liraglutide/
10
(liraglutide or saxenda or victoza or NN2211 or "NN 2211" or "NN-2211").ti,ab.
11
(semaglutide or ozempic or wegovy or NN9535 or "NN 9535" or "NN-9535").ti,ab.
12
(phentermine or Adipex-P or Lomaira or Suprenza).ti,ab.
13
6 or 7 or 8 or 9 or 10 or 11 or 12
14
5 and 13
15
14 not ("address" or "autobiography" or "bibliography" or "biography" or "case reports" or "comment" or
"congress" or "consensus development conference" or "duplicate publication" or "editorial" or
"guideline" or "interview" or "lecture" or "legal case" or "legislation" or "letter" or "news" or "newspaper
article" or "patient education handout" or "periodical index" or "personal narrative" or "portrait" or
"practice guideline" or "review" or "video-audio media").pt.
16
15 not (animals not (humans and animals)).sh.
17
limit 16 to english language
18
remove duplicates from 17
19
limit 18 to ed=20200701-20220330
*Search last updated on July 18, 2022.

©Institute for Clinical and Economic Review, 2022 Page D8
Evidence Report – Medications for Obesity Management Return to Table of Contents
Figure D1. PRISMA Flowchart Showing Results of Literature Search for Medications for Obesity
Management
37 references identified
through other sources
1,408 references after
duplicate removal
115 references assessed
for eligibility in full text
1,421 references
identified through
literature search
1,293 citations excluded
1,408 references screened
63 citations excluded
13 population
19 study design
10 outcomes
21 duplicate data
51 total references
24 RCTs, 2 SLRS
37 references included in
quantitative synthesis

©Institute for Clinical and Economic Review, 2022 Page D9
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Selection
We performed screening at both the abstract and full-text level. A single investigator screened all
abstracts identified through electronic searches according to the inclusion and exclusion criteria
described earlier. We did not exclude any study at abstract-level screening due to insufficient
information. For example, an abstract that did not report an outcome of interest would be
accepted for further review in full text. We retrieved the citations that were accepted during
abstract-level screening for full text appraisal. One investigator reviewed full papers and provided
justification for exclusion of each excluded study.
Data Extraction and Quality Assessment
We used criteria published by the US Preventive Services Task Force to assess the quality of
randomized controlled trials and comparative cohort studies, using the categories “good,” “fair,” or
“poor” (see Table D21).
134
Guidance for quality ratings using these criteria is presented below, as is
a description of any modifications we made to these ratings specific to the purposes of this review.
Good: Meets all criteria: Comparable groups are assembled initially and maintained throughout the
study; reliable and valid measurement instruments are used and applied equally to the groups;
interventions are spelled out clearly; all important outcomes are considered; and appropriate
attention is paid to confounders in analysis. In addition, intention-to-treat analysis is used for
randomized controlled trials.
Fair: Studies were graded "fair" if any or all of the following problems occur, without the fatal flaws
noted in the "poor" category below: Generally comparable groups are assembled initially but some
question remains whether some (although not major) differences occurred with follow-up;
measurement instruments are acceptable (although not the best) and generally applied equally;
some but not all important outcomes are considered; and some but not all potential confounders
are addressed. Intention-to-treat analysis is done for randomized controlled trials.
Poor: Studies were graded "poor" if any of the following fatal flaws exists: Groups assembled
initially are not close to being comparable or maintained throughout the study; unreliable or invalid
measurement instruments are used or not applied equally among groups (including not masking
outcome assessment); and key confounders are given little or no attention. For randomized
controlled trials, intention-to-treat analysis is lacking.
Note that case series are not considered under this rating system – because of the lack of
comparator, these are generally considered to be of poor quality.

©Institute for Clinical and Economic Review, 2022 Page D10
Evidence Report – Medications for Obesity Management Return to Table of Contents
Assessment of Level of Certainty in Evidence
We used the ICER Evidence Rating Matrix to evaluate the level of certainty in the available evidence
of a net health benefit among each of the interventions of focus.
135,136
Assessment of Bias
As part of our quality assessment, we evaluated the evidence base for the presence of potential
publication bias. Given the emerging nature of the evidence base for these newer treatments, we
performed an assessment of publication bias on for semaglutide, liraglutide,
phentermine/topiramate, and bupropion/naltrexone using the ClinicalTrials.gov. We scanned the
site to identify studies which would have met our inclusion criteria and for which no findings have
been published and did not find any evidence of publication bias. We provided qualitative analysis
of the objectives and methods of these studies to ascertain whether there may be a biased
representation of study results in the published literature.
Data Synthesis and Statistical Analyses
The results of the studies were summarized in the evidence tables and described narratively in the
body of the report. In addition, we evaluated the comparative efficacy of semaglutide, liraglutide,
phentermine/topiramate, and bupropion/naltrexone by means of NMA, where feasible. Based on
data availability, our NMA evaluated the outcomes of change in body weight and SBP, and
categorical weight loss at one year. NMA Supplemental Information below contains a detailed
description of the NMA methods. Due to inconsistent or limited data reporting, other outcomes
were only described narratively in the body of the Report and in Section D2.
Supplemental NMA Methods
As described in the Report, we conducted random effect NMAs where feasible. An NMA extends
pairwise meta-analyses by simultaneously combining both the direct estimates (i.e., estimates
obtained from head-to-head comparisons) and indirect estimates (i.e., estimates obtained from
common comparator[s]).
137,138
NMAs were conducted using a Bayesian framework. For continuous outcomes, the NMA model
corresponds to a generalized linear model with identity link.
139
For binary outcomes (e.g.,
proportion of patients discontinuing due to adverse events), the NMA model corresponds to a
generalized linear model with a logit link.
139
For all analyses, we included random effects on the
treatment parameters, and the amount of between-study variance (i.e., heterogeneity) was
assumed constant across all treatment comparisons. We used noninformative prior distributions
for all model parameters. We initially discarded the first 50,000 iterations as “burn-in” and base
inferences on an additional 50,000 iterations using three chains. Convergence of chains was

©Institute for Clinical and Economic Review, 2022 Page D11
Evidence Report – Medications for Obesity Management Return to Table of Contents
assessed visually using trace plots. Furthermore, for any network where there were “loops” in
evidence, we empirically compared the direct and indirect estimates to assess if the NMA
consistency assumption is violated using a node-splitting approach.
139
As there was no evidence of inconsistency, we present the full NMA results in the report. All
analyses were conducted using the IndiRect NMA platform (CRG-EVERSANA, 2020™) or R.
Supplemental NMA Results
We provide three network diagrams that represents the NMAs in the report (Figures D2, D3, and
D4). To interpret the network figures, note that the lines indicate the presence of a trial directly
assessing the connecting interventions, with the thickness of the line corresponding to the number
of trials. The location of treatments and the distances between them do not have any meaning.
The medications are depicted in blue, and the trial names are depicted in orange.
Figure D2. Network of Studies Included in the NMAs of Medications for Obesity, Mean Percentage
Weight Loss, Change in SBP from Baseline to One Year and Categorical Weight Loss
B/N: bupropion/naltrexone, LIR: liraglutide, LSM: lifestyle modification, PBO: placebo, P/T: phentermine/
topiramate, SEM: semaglutide
SEM + LSM
LIR +
LSM
B/N + LSM
P/T + LSM
PBO +
LSM
STEP 1
STEP 5
STEP 8
STEP 8
COR-I
COR-II
SCALE
(Maintenance)
SCALE
(Obesity &
Pre-Diabetes)
STEP 8
EQUIP

©Institute for Clinical and Economic Review, 2022 Page D12
Evidence Report – Medications for Obesity Management Return to Table of Contents
Figure D3. Network of Studies Included in the NMA of Medications for the Management of
Obesity with Diabetes Mellitus, Mean Percentage Weight Loss and Mean Change in SBP from
Baseline to One Year
B/N:
bupropion/naltrexone, LIR: liraglutide, LSM: lifestyle modification, PBO: placebo, P/T: phentermine/ topiramate,
SEM: semaglutide

©Institute for Clinical and Economic Review, 2022 Page D13
Evidence Report – Medications for Obesity Management Return to Table of Contents
Figure D4. Network of Studies Included in the NMAs of Medications for Obesity, Discontinuation
Due to Adverse Events
B/N: bupropion/naltrexone, LIR: liraglutide, LSM: lifestyle modification, PBO: placebo, P/T: phentermine/
topiramate, SEM: semaglutide
Results of Categorical Weight Loss
We conducted NMAs of trials including participants with obesity alone separately from trials of
participants with obesity and diabetes, and excluded trials that included IBT as an adjunct to
medication. Categorical weight loss NMAs (proportion of patients achieving at least 5% or 10%
weight loss) are reported below.
Participants with Obesity Alone
For the trials of the medications conducted in participants with obesity without diabetes that
included standard diet and exercise counseling and reported proportion of patients who achieved
at least 5% or 10% weight loss at one year, we present the results of the baseline risk-adjusted
random effects model, given its better fit for the model compared to the unadjusted model in
Tables D4 and D5. All medications, in combination with diet and exercise counseling, showed
statistically significantly greater odds of achieving at least 5% weight loss at one year. Compared to
SEM + LSM
LIR +
LSM
B/N + LSM
P/T + LSM
PBO +
LSM
STEP 1
STEP 3
STEP 5
STEP 8
STEP 8
COR-I
COR-II
COR-BMOD
SCALE
(Maintenance)
SCALE
(Obesity &
Pre-Diabetes)
STEP 8
SCALE IBT
EQUIP
EQUATE

©Institute for Clinical and Economic Review, 2022 Page D14
Evidence Report – Medications for Obesity Management Return to Table of Contents
placebo, the interventions demonstrated 4.3-17.3 times the odds of 5% weight loss and 3.6-22.4
times the odds of 10% weight loss. Semaglutide demonstrated the greatest odds of achieving 5%
and 10% weight loss at one year and was superior to all other medications in our review for this
outcome. Phentermine/topiramate (high dose) demonstrated greater odds than liraglutide and
bupropion/naltrexone, however this difference was not statistically significant for the outcome of
5% weight loss. Liraglutide was not statistically more effective in demonstrating at least 5% or 10%
weight loss than bupropion/naltrexone (Tables D4 and D5).
Table D4. NMA Results of Medications for the Management of Obesity, Odds Ratio of Likelihood
of Achieving at Least 5% Weight Loss at One Year (95% CI)
Semaglutide
2.0 (0.5 to 10.0)
Phentermine/
Topiramate*
4.0 (2.4 to 8.0) 2.0 (0.6 to 7.1) Liraglutide
4.0 (1.01 to 20.6) 2.0 (0.9 to 4.4) 1.0 (0.3 to 3.4)
Bupropion/
Naltrexone
17.3 (8.9 to 38.3) 8.6 (3.3 to 22.0) 4.3 (2.5 to 6.7) 4.3 (1.7 to 10.2) Placebo
Legend: Each box represents estimated odds ratio of achieving 5% weight loss and 95% credible interval for the
combined direct and indirect comparisons between two medications or one medication and placebo. Estimates in
bold indicate the 95% credible interval does not contain 1.
*High dose.
Table D5. NMA Results of Medications for the Management of Obesity, Odds Ratio of Likelihood
of Achieving at Least 10% Weight Loss at One Year (95% CI)
Semaglutide
2.6 (0.95 to 6.2)
Phentermine/
Topiramate*
5.3 (3.5 to 9.6) 2.1 (1.04 to 5.6) Liraglutide
6.3 (2.4 to 15.9) 2.5 (1.2 to 5.3) 1.2 (0.5 to 2.4)
Bupropion/
Naltrexone
22.4 (13.6 to 36.2) 8.8 (4.7 to 18.1) 4.2 (2.6 to 5.7) 3.6 (2.0 to 6.8) Placebo
Legend: Each box represents estimated odds ratio of achieving 10% weight loss and 95% credible interval for the
combined direct and indirect comparisons between two medications or one medication and placebo. Estimates in
bold indicate the 95% credible interval does not contain 1.
*High dose.

©Institute for Clinical and Economic Review, 2022 Page D15
Evidence Report – Medications for Obesity Management Return to Table of Contents
Participants with Obesity and Diabetes Mellitus
For the trials of the medications conducted in participants with obesity and diabetes mellitus that
included standard diet and exercise counseling and reported proportion of patients who achieved
at least 5% or 10% weight loss at one year, we present the results of the unadjusted random effects
model, given its better fit for the model compared to the baseline-adjusted model in Tables D6 and
D7. Data on categorical weight loss in patients with diabetes mellitus was not available for
phentermine/topiramate and was therefore not included in the NMA. All medications, in
combination with diet and exercise counseling, showed greater odds of achieving at least 5% or
10% weight loss at one year, however, this difference was only statistically significant for liraglutide
for the 5% weight loss outcome and semaglutide and liraglutide for the 10% weight loss outcome.
Compared to placebo, the interventions demonstrated 2.2-2.7 times the odds of 5% weight loss and
3.3-6.1 times the odds of 10% weight loss. Semaglutide demonstrated the greatest odds of
achieving 5% or 10% weight loss at one year, followed by liraglutide.
Table D6. NMA Results of Medications for the Management of Obesity and Diabetes Mellitus,
Odds Ratio of Likelihood of Achieving at Least 5% Weight Loss at One Year (95% CI)
Semaglutide
1.2 (0.4 to 2.9) Liraglutide
1.2 (0.4 to 4.8) 1.1 (0.4 to 4.2)
Bupropion/
Naltrexone
2.7 (0.9 to 4.1) 2.4 (1.0 to 3.6) 2.2 (0.6 to 3.9) Placebo
Legend: Each box represents estimated odds ratio of achieving 5% weight loss and 95% credible interval for the
combined direct and indirect comparisons between two medications or one medication and placebo. Estimates in
bold indicate the 95% credible interval does not contain 1.
Table D7. NMA Results of Medications for the Management of Obesity and Diabetes Mellitus,
Odds Ratio of Likelihood of Achieving at Least 10% Weight Loss at One Year (95% CI)
Semaglutide
1.6 (0.3 to 6.8) Liraglutide
1.8 (0.3 to 12.2) 1.1 (0.2 to 8.1)
Bupropion/
Naltrexone
6.1 (1.3 to 12.8) 3.7 (1.1 to 8.9) 3.3 (0.5 to 10.8) Placebo
Each box represents estimated odds ratio of achieving 10% weight loss and 95% credible interval for the combined
direct and indirect comparisons between two medications or one medication and placebo. Estimates in bold
indicate the 95% credible interval does not contain 1.

©Institute for Clinical and Economic Review, 2022 Page D16
Evidence Report – Medications for Obesity Management Return to Table of Contents
D2. Additional Clinical Evidence
Evidence Base
Semaglutide versus Placebo
The Report discusses the primary sources of data to inform our review of semaglutide for the
management of obesity with and without diabetes mellitus: STEP 1, STEP 2, STEP 3, STEP 5, and
STEP 8 trials. STEP 4 and STEP 6 are two additional trials from the STEP clinical trial program that
were not included in the Report due to study design (STEP 4) and differences in population (STEP 6).
Both studies were multi-center Phase III studies and evaluated subcutaneous semaglutide 2.4 mg
plus lifestyle intervention versus placebo plus lifestyle intervention.
140-142
STEP 6 also evaluated
subcutaneous semaglutide 1.7 mg, but we only reviewed evidence for the subcutaneous
semaglutide 2.4 mg arm as that is the approved dose for obesity treatment.
STEP 4 reported data regarding weight regain, in addition to other outcomes of interest.
Participants included in this trial were adults with BMI ≥30 kg/m
2
or ≥27 kg/m
2
with at least one
weight-related comorbid condition.
140,141
Participants with diabetes mellitus (HbA1C ≥6.5%) were
excluded. The study design included a 20-week run-in period with all participants receiving a dose
escalation of subcutaneous semaglutide starting at 0.25 mg and increased every four weeks to the
maintenance dose of 2.4 mg at week 16. At week 20, subjects were randomized to either continue
semaglutide 2.4 mg or switch to placebo. Due to the withdrawal study design, baseline weight for
these participants was different compared to the STEP trials included in the main review. The
baseline weight and BMI for all participants prior to the run-in period was 107.2 kg and 38.4 kg/m
2
.
At randomization (week 20) baseline weight was 96.5 kg in the semaglutide arm versus 95.4 kg in
the placebo arm and baseline BMI was 34.5 kg/m
2
in the semaglutide arm versus 34.1 kg/m
2
in the
placebo arm (Table D8).
STEP 6 was conducted in Japan and South Korea, with 100% of their participants of Asian
ethnicity.
142
Baseline BMI, body weight, and waist circumference of participants in the STEP 6 trial
were lower than that of the other STEP trials. Additionally, due to differences in guidelines, the
inclusion criteria were slightly different with STEP 6 requiring eligible participants to be adults aged
≥18 in South Korea and ≥20 in Japan with a BMI of at least 27 kg/m
2
with two or more treated or
untreated weight-related comorbidities, or a BMI of at least 35 kg/m
2
with one or more treated or
untreated weight-related comorbidities, according to the Japan Society for the Study of Obesity
(JASSO) guidelines. STEP 6 did not exclude individuals with diabetes mellitus, and at baseline, 25%
of participants in each arm had diabetes mellitus. Outcomes were assessed at week 68 for both
STEP 4 and STEP 6. Baseline characteristics are outlined in Table D8.

©Institute for Clinical and Economic Review, 2022 Page D17
Evidence Report – Medications for Obesity Management Return to Table of Contents
Liraglutide versus Placebo
The Report discusses the primary sources of data to inform our review of semaglutide for the
management of obesity with and without diabetes mellitus: the SCALE clinical trial program
(Maintenance, Obesity & Pre-Diabetes, Sleep Apnea, Type 2 DM, Insulin, and IBT) trials. LOSEIT was
a single-center Phase III trial based at the Parker Institute in Denmark, which evaluated
subcutaneous liraglutide 3.0 mg plus lifestyle intervention versus placebo plus lifestyle
intervention.
143
Participants included in this trial were adults aged 18 to 74 with BMI ≥27 kg/m
2
with symptomatic knee osteoarthritis and were excluded if they were currently using medications
for weight loss or gain, participating in an ongoing weight loss program, or on radiography for end-
stage knee osteoarthritis. Prior to randomization, participants engaged in a dietary intervention
period for eight weeks and were randomized to liraglutide or placebo if they had achieved at least
5% weight-loss during that eight-week period. Baseline characteristics for BMI, weight, and waist
circumference were lower for participants in LOSEIT than those included in the main review.
Primary outcomes for this trial were also slightly different from those included in the main review,
with absolute changes in body weight and Knee Injury and Osteoarthritis Outcome Score (KOOS) as
the co-primary outcomes. The study captured categorical weight loss (≥5% and ≥10%) as well as
change in BMI and waist circumference. Outcomes were assessed at week 52. Baseline
characteristics are outlined in Table D8.
Table D8. Overview of Additional Trials of Semaglutide and Liraglutide for the Management of
Obesity
140-143
STEP 4
STEP 6
LOSEIT
Study Arms
Run-in
PBO*
SEM*
PBO
SEM
PBO
LIR
N
803
268
535
101
199
76
80
Lifestyle Intervention
Monthly counseling, reduced-
calorie diet, and increased
physical activity
Monthly counseling,
reduced-calorie
diet, and increased
physical activity
Low-calorie run-in with
weekly counseling then
reduced-calorie diet, and bi-
weekly counseling for 8
weeks
Mean Age, Years
46
46
47
50
52
59.3
59.2
Female Gender, %
79
76.5
80.2
25.7
42.7
64
65
Baseline
Weight, kg
107.2 95.4 96.5 90.2 86.9 90.8 96.3
Baseline Weight Loss, %
-10.6†
N/A
N/A
N/A
N/A
N/A
N/A
Baseline
BMI, kg/m
2
38.4 34.1 34.5 31.9 32 31.3 32.8
Race, White, %
83.7
84.3
83.4
0
0
NR
NR
Pre-Diabetes, %
NR
NR
NR
25
22
NR
NR
kg: kilogram, LIR: liraglutide, m: meter, N/A: not applicable, N: total number, NR: not reported, PBO: placebo, SEM:
semaglutide
*Baseline data measured at Week 20.
†Change from baseline data measured at Week 20.

©Institute for Clinical and Economic Review, 2022 Page D18
Evidence Report – Medications for Obesity Management Return to Table of Contents
Phentermine/Topiramate versus Placebo
The Report discusses the primary source of data to inform our review of phentermine/topiramate
for the management of obesity: the EQUIP and EQUATE trials. OB-204 was a single-center, double-
blind, parallel-group, placebo-controlled, Phase I/II trial that randomized adults with overweight or
obesity and moderate-to-severe obstructive sleep apnea syndrome to receive phentermine 15
mg/topiramate 92 mg (n=22), or placebo (n=23) (Table D9).
144
All participants in each treatment
group also received standardized lifestyle modification counseling. Participants were eligible to
participate if they were between the ages of 30-65 years, had a BMI of 30-40 kg/m
2
, a diagnosis of
moderate-to-severe obstructive sleep apnea syndrome, an apnea-hypopnea index ≥15, and were
unable to comply with CPAP treatment. Participants were excluded if they had a sleep disorder
other than obstructive sleep apnea syndrome, unstable angina or heart failure, history of
myocardial infarction, coronary revascularization, cholecystitis or cholelithiasis, glaucoma, or
seizures, used any prescription central nervous system stimulant, experienced a weight change >5
kg, had previous surgery for obesity, had a psychiatric disorder, or were pregnant or breastfeeding.
Participants in the OB-204 trial had a mean age of 52 years, and 47% were female. The majority
(91%) of participants were White and 9% were Black. The average weight of participants in this trial
was 105 kg and mean BMI was 36 kg/m
2
at baseline. See Table D9 for detailed baseline
characteristics.
Bupropion/Naltrexone versus Placebo
The Report discusses the primary sources of data to inform our review of bupropion/naltrexone for
the management of obesity: COR-I, COR-II and COR-BMOD. CVOT Light was a multi-center, Phase
IIIb trial that randomized participants with overweight or obesity at an increased risk of adverse
cardiovascular outcomes to receive bupropion 360 mg/naltrexone 32 mg or placebo.
145,146
All
participants in each treatment arm were also encouraged to participate in an Internet-based weight
management program that included resources on healthy eating such as a low-calorie mean plan,
exercise, behavioral modifications, weekly lessons, and access to a personal coach. Participants
were eligible to participate if they were women over 50 years old, or men over 45 years old, had a
BMI of 27-50 kg/m
2
, a waist circumference of ≥88 cm for women or ≥102 cm for men, and
demonstrated an increased risk of adverse cardiovascular outcomes, such as confirmed or high
likelihood of cardiovascular disease, or had type 2 diabetes mellitus and at least two of the
following: hypertension, dyslipidemia requiring pharmacotherapy, low high-density lipoprotein
cholesterol, or were currently smoking tobacco. Participants were excluded if they had a
myocardial infarction within four months, severe angina pectoris, NYHA class III or IV heart failure,
history of stoke or SBP ≥145 mmHg or diastolic blood pressure ≥95 mmHg, weight change >3%
within three months, had surgery for obesity, or history of seizures, mania, psychosis, bulimia, or
anorexia nervosa. Participants in CVOT Light had a mean age of 61 years, and 55% were female.

©Institute for Clinical and Economic Review, 2022 Page D19
Evidence Report – Medications for Obesity Management Return to Table of Contents
The majority (84%) of participants were White and 15% were Black. The average weight of
participants in this trial was 106 kg and mean BMI was 37 kg/m
2
at baseline (Table D9).
Ignite was a multi-center, open-label, Phase IIIb trial that randomized participants for the first 26
weeks to receive bupropion 360 mg/naltrexone 32 mg or usual care.
147
Participants in the
treatment arm were additionally required to participate in a comprehensive lifestyle intervention,
which consisted of a progressive nutrition and exercise program with personalized goal-setting and
tracking tools with a coach or dietitian, while participants in the usual care arm were instructed to
follow an exercise prescription and a hypocaloric diet. From 26 weeks through 78 weeks,
participants in the bupropion/naltrexone group continued on the medication, while participants in
usual care arm were switched to bupropion/naltrexone in addition to the comprehensive lifestyle
intervention. For the purposes of our review, we are evaluating efficacy data only up to 26 weeks
because of the lack of comparative data beyond that timepoint. Participants were eligible to
participate if they were between the ages of 18-60 years, had either a BMI of 30-45 kg/m
2
or a BMI
27-45 kg/m
2
with dyslipidemia and/or controlled hypertension. Participants were excluded if they
had type 1 or type 2 diabetes mellitus, myocardial infarction within six months, angina pectoris
grade III/IV, history of strokes, seizures, bulimia, anorexia nervosa, had surgery for obesity, or had a
psychiatric illness including mania, psychosis, or depression. Participants in this trial had a mean
age of 47 years and were predominantly female (84%). The majority (76%) of participants were
White and 23% were Black. The average weight of participants in this trial was 101 kg and mean
BMI was 36 kg/m
2
at baseline. See Table D9 for detailed baseline characteristics.

©Institute for Clinical and Economic Review, 2022 Page D20
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D9. Overview of Additional Trials of Phentermine/Topiramate and Bupropion/Naltrexone
for the Management of Obesity
144-149
OB-204
CVOT Light
Ignite
Study Arms
PBO
P/T (high)
PBO
B/N
PBO
B/N
N
23
22
4,450
4,455
89
153
Lifestyle
Intervention
LSM counseling,
reduced-calorie diet,
and increased physical
activity
LSM counseling,
reduced-calorie diet,
and increased physical
activity
LSM counseling,
reduced-calorie
diet, and
increased physical
activity
CLI with progressive
nutrition and an
exercise program,
and personalized
goal-setting
Mean Age,
Years
51.4 53.4 60.9 61.1 47 46.1
Female
Gender, %
34.8 59.1 54.4 54.7 86.5 81.7
Baseline
Weight, kg
106.9 103.7 106.3 105.6 100.2 101.4
Baseline
BMI, kg/m
2
35.3 36 37.4 37.2 36.3 36.3
Race,
White, %
91.3 90.9 83.1 83.9 71.9 81
Pre-
Diabetes, %
NR NR NR NR NR NR
B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, kg: kilogram, LSM: lifestyle modification, m:
meter, N: total number, NR: not reported, PBO: placebo, P/T: phentermine/topiramate
Results
For each medication, secondary outcomes from trials in the Report are summarized first, followed
by primary outcomes for the additional trials summarized in the supplement. Weight loss
outcomes are summarized first, followed by other outcomes (e.g., waist circumference, blood
glucose, and LDL cholesterol), where relevant. HRQoL is summarized for all drugs at the end of this
section. For each medication, results of trials conducted in patients with obesity are presented first,
followed by trials conducted in patients with obesity and diabetes mellitus.
Semaglutide versus Placebo
The efficacy of semaglutide compared with placebo for the management of obesity in patients
without diabetes mellitus was evaluated in three Phase III trials (STEP 1, 3, and 5). We were able to
obtain percent weight loss at six months through digitizing published graphical data. Participants in
the subcutaneous semaglutide 2.4 mg arm achieved greater percent weight loss at six months
(-11.7%, -15.4%, and -13.2% respectively) compared to placebo (-2.9%, -7.9%, and -2.6%,
respectively).
29,31,34-38,143
Similarly, at one year, the proportion of participants who achieved at least
15% weight loss and at least 20% weight loss, a greater proportion of participants in the
semaglutide arm achieved these categorical outcomes compared to participants in the placebo.
Treatment with semaglutide in STEP 1, 3, and 5 trials also resulted in additional clinical benefits in

©Institute for Clinical and Economic Review, 2022 Page D21
Evidence Report – Medications for Obesity Management Return to Table of Contents
waist circumference, blood glucose, and LDL cholesterol compared to placebo. Outcomes related
to changes in LDL were reported as absolute change from baseline for STEP 3 and as ratio of LDL
from baseline for STEP 1 and 5. See Table D10 for detailed results.
Additionally, in an extension trial of STEP 1, participants went off semaglutide treatment at week 68
and were evaluated through the end of the trial at week 120. At that timepoint, participants who
were initially taking semaglutide, but went off-treatment, regained 14.8% of their weight from
week 68, and participants who were initially on placebo regained 2.1% of their weight.
72
In the
initial semaglutide arm, nearly two-thirds of the weight participants lost from baseline was regained
in about a year. Similarly, metabolic parameters, such as blood pressure and HbA1C, returned to
baseline values at the end of the trial. See Tables D26-D29 for detailed results.
The efficacy of semaglutide for the management of obesity and type 2 diabetes mellitus was
evaluated through one Phase III trial (STEP 2). We were able to obtain percent weight loss at six
months through digitizing published graphical data. Participants in the subcutaneous semaglutide
2.4 mg arm achieved greater percent weight loss at six months (-8.7%) compared to placebo
(-2.7%) (Table D12).
30
Similarly, at one year, the proportion of participants who achieved at least
15% weight loss and at least 20% weight loss, a greater proportion of participants in the
semaglutide arm ([15% WL: 25.8%]; [20% WL: 13.1%]) achieved these categorical outcomes
compared to participants in the placebo arm ([15% WL: 3.2%]; [20% WL: 1.6%]). Treatment with
subcutaneous semaglutide 2.4 mg was also associated with greater improvements in waist
circumference (-9.4 cm) compared to placebo (-4.5 cm). There were no clinical differences between
the subcutaneous semaglutide 2.4 mg arm and placebo arm in blood glucose and LDL cholesterol.
STEP 4, which had a crossover design including a 20-week run-in semaglutide dose escalation prior
to randomization to either continue subcutaneous semaglutide 2.4 mg or switch to placebo,
assessed the efficacy of semaglutide compared with placebo for the management of obesity.
140,141
Prior to randomization, all participants achieved a mean weight loss of -10.6% in the 20-week run-in
period. After randomization, at one year, participants in the subcutaneous semaglutide 2.4 mg arm
achieved additional weight loss (-7.9%) compared to participants in the placebo arm who
experienced weight regain (6.9%). More participants who switched to placebo experienced weight
regain (81.2%) compared to those who continued on semaglutide (12.3%). Overall percent weight
loss at one year from week 0 (including semaglutide run-in) was -17.8% in the semaglutide arm
compared to -5.4% in the placebo arm. For the co-primary outcomes of proportion of participants
who achieved at least 5%, 10%, 15%, or 20% weight loss at one year, a greater proportion of
participants in the semaglutide arm (88.7%, 79%, 63.7%, and 39.6%, respectively) achieved each
categorical outcome compared to participants in the placebo arm (47.6%, 20.4%, 9.2%, and 4.8%,
respectively). These categorical outcome data are digitized from published graphical data. See
Table D13 for detailed results.

©Institute for Clinical and Economic Review, 2022 Page D22
Evidence Report – Medications for Obesity Management Return to Table of Contents
STEP 6 evaluated the efficacy of semaglutide compared with placebo for the management of
obesity in patients with or without diabetes mellitus. Participants in the subcutaneous semaglutide
2.4 mg arm achieved greater percent weight loss at one year (-13.2%) compared to placebo
(-2.1%) (Table D13).
142
Similarly, for the co-primary outcomes of proportion of participants who
achieved at least 5%, 10%, 15%, or 20% weight loss at one year, a greater proportion of participants
in the semaglutide arm (83%, 61%, 41%, and 20%, respectively) achieved each categorical outcome
compared to participants in the placebo arm (21%, 5%, 3%, and 2%, respectively).
Semaglutide versus Liraglutide
The efficacy of subcutaneous semaglutide versus subcutaneous liraglutide with a placebo
comparator for the management of obesity was evaluated in one Phase III trial (STEP 8).
33
We were
able to obtain percent weight loss at six months for the semaglutide and liraglutide arms by
digitizing published graphical data. Data on weight loss at six months were not available for the
placebo arm. Participants in the semaglutide arm achieved greater percent weight loss at six
months (-13.3%) compared to participants in the liraglutide arm (-6.8%). Treatment with
semaglutide also resulted in additional clinical benefits in waist circumference, blood glucose, and
LDL cholesterol compared to both liraglutide and placebo. Treatment with liraglutide resulted in
additional clinical benefits in waist circumference and blood glucose compared to placebo;
however, participants in the liraglutide arm experienced an increase in LDL cholesterol from
baseline (0.9 mg/dL) compared to semaglutide (-6.5 mg/dL) and placebo (-1.1 mg/dL), which both
had reduced LDL cholesterol from baseline. See Table D10 for detailed results.

©Institute for Clinical and Economic Review, 2022 Page D23
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D10. Secondary Outcomes of Key Trials of Semaglutide for the Management of
Obesity
29,31,33-38
STEP 1
STEP 3
STEP 5
STEP 8
Study Arms
PBO
SEM
PBO
SEM
PBO
SEM
PBO
SEM
LIR
N
577
1,212
189
373
129
149
78
117
117
% Weight Loss from
Baseline to 6 Months,
Mean (SE)
-2.9*
(0.2)
-11.7*
(0.2)
-7.9
(0.5)†
-15.4*
(0.3)†
-2.6
(NR)
-13.2
(NR)
NR
-13.3*
(NR)
-6.8*
(NR)
Participants with 15%
Weight loss, n (%)
28
(4.9)
612
(50.5)
25
(13.2)
208
(55.8)
7 (5.4)
78
(52.3)
5 (6.4)
65
(55.6)
14
(12)
Participants with 20%
Weight loss, n (%)
10
(1.7)
388
(32)
7
(3.7)
133
(35.7)
3 (2.3)
52
(34.9)
2 (2.6)
45
(38.5)
7 (6)
Change in Waist
Circumference, cm,
Mean (SE)
-4.1
(NR)
-13.5
(NR)
-6.3
(NR)
-14.6
(NR)
-4.5
(0.6)†
-14.3
(0.8)†
-2
(1.1)†
-13.2
(0.9)†
-6.6
(0.9)†
Change in Fasting
Blood Glucose, mg/dL,
Mean (SE)
-0.5
(NR)
-8.4
(NR)
-0.7
(NR)
-6.7
(NR)
1.6§
(NR)
-7.6§
(NR)
3.3
(1.4)†
-8.3
(1.1)†
-4.3
(1.2)†
Change in LDL
Cholesterol, mg/dL,
Mean (SD)
1.1*‡
(NR)
-3.3*‡
(NR)
2.6*
(NR)
-4.7
(NR)
-1.1‡
(NR)
-7.8‡
(NR)
-1.1*
(5.6)†
-6.5*
(3.1)†
0.9*
(2.8)†
cm: centimeter, dL: deciliter, LDL: low-density lipoprotein, LIR: liraglutide, mg: milligram, n: number, N: total
number, NR: not reported, PBO: placebo, SBP: systolic blood pressure, SD: standard deviation, SE: standard error,
SEM: semaglutide
*The number of patients for this outcome may differ from the primary analysis population.
†SE manually derived from standard deviation or 95% CIs.
‡Change in LDL cholesterol was calculated using ratio of LDL and respective baseline LDL.
§Timepoint for this outcome is at Week 104.
Liraglutide versus Placebo
The efficacy of liraglutide compared with placebo for the management of obesity was evaluated in
four Phase III trials in the SCALE clinical trial program (Maintenance, Sleep Apnea, Obesity & Pre-
Diabetes, IBT). We were able to obtain percent weight loss at six months by digitizing published
graphical data. Participants in the liraglutide arms achieved greater percent weight loss at six
months (-7.7%, -5.7%, -8.2%, and -8.4%) compared to participants in the placebo arm (-1%, -1.6%, -
2.9%, and -5.4%).
40,41,43,44,48-51
Data for the co-primary outcome of proportion of participants who
achieved at least 15% weight loss at one year were only available for SCALE (IBT), in which a greater
proportion of participants in the liraglutide arm (18.1%) achieved the outcome compared to the
placebo arm (8.9%). Treatment with liraglutide resulted in additional benefits in waist
circumference and blood glucose compared to placebo. Treatment with liraglutide resulted in
additional benefits in LDL cholesterol in the Obesity & Pre-Diabetes (-3 mg/dL) and IBT (-1.5 mg/dL)
trials compared to placebo (-1 mg/dL and 1.5 mg/dL, respectively). In the Maintenance trial,
participants in both the liraglutide and placebo arms experienced an increase in LDL cholesterol
from baseline (7.7 mg/dL and 11.6 mg/dL, respectively), although there was a greater increase in

©Institute for Clinical and Economic Review, 2022 Page D24
Evidence Report – Medications for Obesity Management Return to Table of Contents
the placebo arm. Data on LDL cholesterol were not available for the Sleep Apnea trial. See Table
D11 for detailed results.
The efficacy of subcutaneous liraglutide 3.0 mg compared with placebo for the management of
obesity with diabetes mellitus was evaluated in two Phase III trials in the SCALE clinical trial program
(Type 2 Diabetes, Insulin).
42,45,52
We were able to obtain percent weight loss at six months through
digitizing published graphical data. Participants in the liraglutide arms achieved greater percent
weight loss at six months (-6% and -6.4%, respectively) compared to participants in the placebo arm
(-2.7% and -2.1%, respectively) (Table D12). Categorical data for proportion of participants who
achieved at least 15% weight loss at one year were not available for either study. Treatment with
liraglutide resulted in additional benefits in waist circumference and blood glucose compared to
placebo. In the Type 2 Diabetes trial, participants in both the liraglutide and placebo arms
experienced an increase in LDL cholesterol from baseline (0.6 mg/dL and 5 mg/dL, respectively).
Participants receiving liraglutide in the Insulin trial improved in LDL cholesterol from baseline (-2.8
mg/dL) compared to participants in the placebo arm, who experienced an increase in LDL
cholesterol (0.9 mg/dL).
LOSEIT evaluated the efficacy of liraglutide compared with placebo for the management of obesity
in patients with or without diabetes mellitus. Data for percent weight loss at one year were not
available. For the co-primary outcomes of proportion of participants who achieved at least 5%
weight loss and at least 10% weight loss at one year, a great proportion of participants in the
liraglutide arm achieved each categorical outcome (35% and 21.3%, respectively) compared to
participants in the placebo arm (17.1% and 9.6%, respectively).
143
See Table D13 for detailed
results.

©Institute for Clinical and Economic Review, 2022 Page D25
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D11. Secondary Outcomes of Key Trials of Liraglutide for the Management of
Obesity
40,41,43,44,48-51
SCALE
Maintenance
SCALE
Sleep Apnea‡
SCALE Obesity &
Pre-Diabetes
SCALE IBT
Study Arms
PBO
LIR
PBO
LIR
PBO
LIR
PBO
LIR
N
206
207
178
175
1,225
2,437
130
141
% Weight Loss from
Baseline to 6
Months, Mean (SE)
-1* (0.5)
-7.7*
(0.5)
-1.6
(0.3)
-5.7
(0.4)
-2.9
(0.3)
-8.2
(0.2)
-5.4*
(0.5)
-8.4*
(0.6)
Participants with
15% Weight loss, n
(%)
NR NR NR NR NR NR 12 (8.9)
26
(18.1)
Change in Waist
Circumference, cm,
Mean (SE)
-1.2
(0.4)†
-4.7
(0.5)†
-3.1
(0.5)
-6.4
(0.5)
-3.9
(0.2)†
-8.2
(0.1)†
-6.7
(NR)
-9.4
(NR)
Change in Fasting
Blood Glucose,
mg/dL, Mean (SE)
-3.6
(0.9)†
-9.0
(0.8)†
3.6 (1.8)
-3.6
(1.8)
0.1
(0.3)†
-7.1
(0.2)†
0.2 (NR)
-4.1
(NR)
Change in LDL
Cholesterol, mg/dL,
Mean (SD)
11.6
(1.6)†
7.7
(1.6)†
NR NR -1 (NR) -3 (NR) 1.5 (NR)
-1.5
(NR)
cm: centimeter, dL: deciliter, LDL: low-density lipoprotein, LIR: liraglutide, mg: milligram, n: number, N: total
number, NR: not reported, PBO: placebo, SBP: systolic blood pressure, SD: standard deviation, SE: standard error
*The number of patients for this outcome may differ from the primary analysis population.
†SE manually derived from standard deviation or 95% CIs.
‡Timepoint for all outcomes except percent weight loss is at week 32.

©Institute for Clinical and Economic Review, 2022 Page D26
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D12. Secondary Outcomes of Key Trials of Semaglutide and Liraglutide for the Management
of Obesity with Diabetes Mellitus
30,42,45,52
STEP 2
SCALE
Type 2 Diabetes
SCALE
Insulin
Study Arms
PBO
SEM
PBO
LIR
PBO
LIR
N
376
388
211
412
193
191
% Weight Loss from
Baseline to 6 Months,
Mean (SE)
-2.7* (0.2) -8.7* (0.3) -2.7* (0.3)‡ -6* (0.3)‡
-2.1*
(0.4)
-6.4* (0.4)
Participants with 15%
Weight loss, n (%)
12 (3.2) 100 (25.8) NR NR NR NR
Participants with 20%
Weight loss, n (%)
6 (1.6) 51 (13.1) NR NR NR NR
Change in Waist
Circumference, cm,
Mean (SE)
-4.5 (0.4) -9.4 (0.4) -2.7 (0.4)‡ -6.1 (0.3)‡ -2.6 (NR) -5.3 (NR)
Change in Fasting Blood
Glucose, mg/dL, Mean
(SE)
-0.1 (1.8) -2.1 (1.8) -0.2 (2.5)‡ -34.3 (1.9)‡
-11.5
(NR)
-18.4 (NR)
Change in LDL
Cholesterol, mg/dL,
Mean (SD)
0* (NR)† 0* (NR)† 5 (NR) 0.6* (NR)
0.9*
(NR)†
-2.8*
(NR)†
cm: centimeter, dL: deciliter, LDL: low-density lipoprotein, mg: milligram, n: number, N: total number, NR: not
reported, PBO: placebo, SBP: systolic blood pressure, SD: standard deviation, SE: standard error, SEM: semaglutide
*The number of patients for this outcome may differ from the primary analysis population.
†Change in LDL cholesterol was calculated using ratio of LDL and respective baseline LDL.
‡SE manually derived from standard deviation or 95% CIs.

©Institute for Clinical and Economic Review, 2022 Page D27
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D13. Results of Additional Trials of Semaglutide and Liraglutide for the Management of
Obesity
140-143
STEP 4
STEP 6
LOSEIT
Study Arms
PBO
SEM
PBO
SEM
PBO
LIR
N
250
520
100
193
76
80
% Weight Loss from
Baseline to One Year, Mean
(SE)
6.9*‡
(0.5)†
-7.9*‡ (4)† -2.1 (0.8) -13.2 (0.5) NR NR
Participants with at Least
5% Weight Loss, n (%)
119§
(47.6)
461§ (88.7) 21 (21) 160 (83) 13 (17.1) 28 (35)
Participants with at Least
10% Weight Loss, n (%)
51§
(20.4)
411§ (79) 5 (5) 117 (61) 7 (9.6) 17 (21.3)
Participants with at Least
15% Weight Loss, n (%)
23§ (9.2) 331§ (63.7) 3 (3) 79 (41) NR NR
Participants with at Least
20% Weight Loss, n (%)
12§ (4.8) 206§ (39.6) 2 (2) 38 (20) NR NR
LIR: liraglutide, n: number, N: total number, NR: not reported, PBO: placebo, SEM: semaglutide
*The number of patients for this outcome may differ from the primary analysis population.
†SE manually derived from standard deviation or 95% CIs.
‡Timepoint for this outcome is Weeks 20-68.
§Timepoint for this outcome is Weeks 0-68.
Phentermine/Topiramate versus Placebo
The Report discusses the primary outcome of percentage weight loss at one year and proportion of
participants achieving 5% and 10% weight loss in the EQUIP trial. In the EQUIP trial, data on weight
loss at six months were not available. For the categorical outcome of at least 15% weight loss at
one year, more participants in the phentermine 15 mg/topiramate 92 mg arm achieved this
outcome (32%) compared to those in placebo (3%)
54-57
(Table D14). In EQUATE, at six months,
participants in the high-dose phentermine/topiramate arm experienced the greatest percent
weight loss from baseline (-9.2%), followed by the low-dose intervention arm (-8.5%), and placebo
(-1.7%). Categorical weight loss of at least 15% at one year was not assessed in the EQUATE trial.
Treatment with phentermine/topiramate in both EQUIP and EQUATE was associated with
additional clinical benefits in terms of reductions in waist circumference, blood glucose, and LDL
cholesterol at one year. In the EQUIP trial, mean reduction in waist circumference was greater in
the treatment arm than placebo (-10.9 cm vs. -3.1cm, respectively).
54-57
Mean reduction in waist
circumference in the high-dose and low-dose intervention arms in EQUATE was also greater than
placebo (-8.7 cm and -8.8 cm, versus -3.1cm, respectively). In the EQUIP trial, participants receiving
phentermine/topiramate experienced a small improvement in their blood glucose levels (-0.6
mg/dL), while participants receiving placebo experienced a slight elevation in blood glucose on
average (1.9 mg/dL). Participants in both arms improved LDL cholesterol levels, but the effect was
greater in the phentermine/topiramate arm (-8.4 vs. -5.5 mg/dL, respectively). In the EQUATE trial,

©Institute for Clinical and Economic Review, 2022 Page D28
Evidence Report – Medications for Obesity Management Return to Table of Contents
mean change from baseline in blood glucose levels in both arms was negligible (-1 to 0 mg/dL
change). See Table D14 for detailed results.
In the diabetes mellitus subgroup of the CONQUER trial, data on secondary outcomes such as
weight loss at six months, categorical weight loss of at least 15%, and change in waist circumference
were not available. All reported outcomes here are from the one-year timepoint. Participants in
the diabetes subgroup receiving high-dose and low-dose phentermine/topiramate experienced a
greater improvement in their blood glucose levels than participants in the placebo group (-12.6 and
-9 vs. -5.4 mg/dL, respectively).
53,58
Similar trends were observed for LDL cholesterol; high and low-
dose phentermine/topiramate was associated with greater improvements in LDL compared to
placebo (-2.8 and -3.6 vs. -2.3 mg/dL, respectively). See Table D15 for detailed results.
In the Phase I/II OB-204 trial, efficacy outcomes were assessed at 28 weeks. At that timepoint,
participants in the phentermine/topiramate arm achieved a greater percent weight loss (-10.3%)
compared to participants in the placebo arm (-4.2%).
144
Similarly, more participants receiving the
intervention achieved target weight loss of at least 5% and 10% body weight than participants
receiving placebo. See Table D16 for detailed results.
Bupropion/Naltrexone versus Placebo
Weight loss data at six months were not available in the COR-I trial. In COR-II and COR-BMOD,
participants in the bupropion/naltrexone arms experienced greater weight loss than participants in
the placebo arms at six months (-6.5% and -9.4% vs. -1.9% and -5.6%, respectively) (Table D14).
Similarly, for all three trials, more participants in the treatment arms achieved at least 15%
bodyweight at one year compared to the placebo arms.
63-66
At the one-year timepoint, participants receiving bupropion/naltrexone in the COR-I, COR-II, and
COR-BMOD trials experienced greater improvement in waist circumference (-6.2, -6.7, and -10 cm,
respectively) than participants receiving placebo (-2.5, -2.1, and -6.8, respectively).
61-66
Similarly,
participants receiving bupropion/naltrexone achieved greater improvements in blood glucose levels
(-3.2, -2.8, and -2.4 mg/dL) versus placebo (-1.3, -1.3, and -1.1, respectively). In COR-I and COR-II,
participants in the intervention arms experienced a greater improvement from baseline in their LDL
cholesterol (-4.4 and -6.2 mg/dL, respectively), compared to placebo (-3.3 and -2.1 mg/dL,
respectively). However, in the COR-BMOD trial, both arms experienced an increase in their LDL
cholesterol, with participants in the placebo arm experiencing a greater increase (8.1 mg/dL) than
participants in the bupropion/naltrexone arm (5.4 mg/dL). See Table D14 for detailed results.
In the COR Diabetes trial of bupropion/naltrexone for the management of obesity with diabetes
mellitus, participants in the intervention arm experienced a greater percent change in their weight
at six months (-5.1%) compared to those in the placebo arm (-2%).
59,60
Categorical weight loss of at
least 15% at one year was not available in this trial. At the one-year timepoint, participants in the

©Institute for Clinical and Economic Review, 2022 Page D29
Evidence Report – Medications for Obesity Management Return to Table of Contents
treatment arm experienced greater improvements in waist circumference compared to placebo (-5
cm vs. -2.9 cm, respectively), change in blood glucose (-11.9 mg/dL vs. -4 mg/dL, respectively) and
change in LDL cholesterol (-1.4 mg/dL vs. 0 mg/dL, respectively). See Table D15 for detailed results.
In CVOT Light, participants in the bupropion 360 mg/naltrexone 32 mg arm achieved greater weight
loss at one year (-4.6%) than participants in the placebo arm (-1.8%) (Table D16).
145,146
The
categorical weight loss outcomes of at least 5% and 10% were not assessed in this trial.
In the Ignite trial, since all participants were either switched or continued on open-label
bupropion/naltrexone treatment at 26 weeks, we evaluated efficacy outcomes only up to that
timepoint.
147,149
Similar to CVOT Light, participants in the intervention arm achieved a greater
weight improvement at week 26 (-9.5%) compared to participants in the usual care arm (-0.9%).
For the endpoint of proportion of participants who lost at least 5% of and 10% of their weight, more
participants in the bupropion/naltrexone treatment arm achieved these outcomes compared to
participants in the usual care group. See Table D16 for detailed results.
Table D14. Secondary Outcomes of Key Trials of Phentermine/Topiramate and
Bupropion/Naltrexone for the Management of Obesity
54-57,61-66,85
EQUIP
EQUATE
COR-I
COR-II
COR BMOD
Study Arms PBO
P/T
(high)
PBO
P/T
(low)
P/T
(high)
PBO B/N PBO B/N PBO B/N
N
498
498
103
103
103
511
471
456
702
193
482
% Weight Loss
from Baseline to
6 Months, Mean
(SE)
NR NR
-1.7
(0.6)
-8.5
(0.6)
-9.2
(0.6)
NR NR
-1.9*
(0.3)
-6.5*
(0.2)
-5.6*
(0.5)
-9.4*
(0.4)
Participants with
15% Weight loss,
n (%)
17
(3.4)
161
(32.3)
NR NR NR 10 (2)
56
(12)
11
(2.4)
95
(13.5)
21
(10.9)
140
(29.1)
Change in Waist
Circumference,
cm, Mean (SE)
-3.1
(0.5)†
-10.9
(0.5)†
-3.3
(0.7)
-8.8*
(0.7)
-8.7
(0.7)
-2.5
(0.4)
-6.2
(0.4)
-2.1
(0.5)
-6.7
(0.3)
-6.8
(0.8)
-10
(0.5)
Change in
Fasting Blood
Glucose, mg/dL,
Mean (SE)
1.9
(0.5)†
-0.6
(0.5)†
-0.1*
(0.1)
0*
(0.1)
-0.1*
(0.1)
-1.3
(0.6)
-3.2
(0.6)
-1.3
(0.6)
-2.8
(0.5)
-1.1
(1)
-2.4
(0.6)
Change in LDL
Cholesterol,
mg/dL, Mean
(SD)
-5.5*
(0.9)†
-8.4*
(0.9)†
NR NR NR
-3.3*
(1.2)
-4.4*
(1.2)
-2.1*
(1.3)
-6.2*
(0.9)
8.1*
(2.1)
5.4*
(1.4)
B/N: bupropion/naltrexone, cm: centimeter, dL: deciliter, LDL: low-density lipoprotein, LIR: liraglutide, mg:
milligram, n: number, N: total number, NR: not reported, PBO: placebo, P/T: phentermine/topiramate, SBP:
systolic blood pressure, SD: standard deviation, SE: standard error
*The number of patients for this outcome may differ from the primary analysis population.
†SE manually derived from standard deviation or 95% CIs.

©Institute for Clinical and Economic Review, 2022 Page D30
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D15. Secondary Outcomes of Key Trials of Phentermine/Topiramate and
Bupropion/Naltrexone for the Management of Obesity and Obesity with Diabetes
53,58-60
CONQUER (Diabetes Subgroup)
COR Diabetes
Study Arms
PBO
P/T (low)
P/T (high)
PBO
B/N
N
157
67
164
159
265
% Weight Loss from
Baseline to 6 Months, Mean
(SE)
NR NR NR -2* (0.4) -5.1* (0.3)
Participants with 15%
Weight loss, n (%)
NR NR NR NR NR
Change in Waist
Circumference, cm, Mean
(SE)
NR NR NR -2.9 (0.6) -5 (0.5)
Change in Fasting Blood
Glucose, mg/dL, Mean (SE)
-5.4 (1.8)† -9 (3.6)† -12.6 (1.8)† -4 (3.4) -11.9 (2.7)
Change in LDL Cholesterol,
mg/dL, Mean (SD)
-2.3* (2.1) -3.6* (3.2) -2.8* (2) 0* (2.4) -1.4* (1.9)
B/N: bupropion/naltrexone, cm: centimeter, dL: deciliter, LDL: low-density lipoprotein, LIR: liraglutide, mg:
milligram, n: number, N: total number, NR: not reported, PBO: placebo, P/T: phentermine/topiramate, SBP:
systolic blood pressure, SD: standard deviation, SE: standard error
*The number of patients for this outcome may differ from the primary analysis population.
†SE manually derived from standard deviation or 95% CIs.
Table D16. Results of Additional Trials of Phentermine/Topiramate and Bupropion/Naltrexone for
the Management of Obesity
144-149
OB-204†
CVOT Light
Ignite‡
Study Arms PBO
P/T
(high)
PBO B/N PBO B/N
N
23
22
4450
4455
82
71
% Weight Loss
from Baseline to
One Year, Mean
(SE)
-4.2 (1.2)
-10.3
(1.2)
-1.8* (NR) -4.6* (NR) -0.9 (0.5) -9.5 (0.5)
Participants with
5% Weight Loss, n
(%)
11 (47.8) 16 (72.7) NR NR 10 (12.2) 60 (84.5)
Participants with
10% Weight Loss,
n (%)
3 (13) 12 (54.5) NR NR 3 (3.7) 30 (42.3)
B/N: bupropion/naltrexone, n: number, N: total number, NR: not reported, PBO: placebo, P/T:
phentermine/topiramate, SE: standard error
*The number of patients for this outcome may differ from the primary analysis population.
†Timepoint for all outcomes is at week 28.
‡Timepoint of interest for all outcomes for this trial is at week 26.

©Institute for Clinical and Economic Review, 2022 Page D31
Evidence Report – Medications for Obesity Management Return to Table of Contents
HRQoL
As discussed in the Report, HRQoL was assessed using a variety of instruments, including SF-36v2,
IWQOL-Lite, PHQ-9, and IDS-SR. SF-36v2 consists of 36 questions across eight domains, including
physical functioning. Additionally, SF-36v2 provides two aggregated scores: the physical
component summary (PCS) and mental component summary (MCS). For the SF-36v2 and IWQOL-
Lite-CT instruments, an increase in score is representative of an improvement in health status
(positive is better). The PHQ-9 and IDS-SR and reflect depressive symptom severity; a decrease in
score in these measures indicates an improvement in depressive symptoms (lower is better).
For each medication, HRQoL data for additional studies included in the Supplement are described in
the text below. Additional HRQoL data beyond physical functioning and mental scores for studies
from the Report are also discussed in the text below. The Report outlines physical function and
mental HRQoL data for studies included in our primary analysis. Data from the Report for physical
function and mental HRQoL are outlined in Tables D17 and D18 below.
Semaglutide
HRQoL in STEP 4 was assessed using the SF-36v2 physical function score. During the 20-week run-in
period, participants experienced an average score improvement of 2.2 from baseline score. After
randomization, from weeks 20 to 68, participants who continued semaglutide experienced a further
improvement in physical functioning score (1.0) compared to a decreased score for those who
switched to placebo (-1.5). Additionally, improvements were seen in the semaglutide arm for the
SF-36v2 Physical Component Summary (0.8) and Mental Component Summary (0.1) compared to
decreased scores for both in the placebo arm (-0.9 and -3.4, respectively).
140
(Table D30).
Patient reported outcomes for STEP 6 included SF-36v2 physical functioning scores and the IWQOL-
Lite-CT physical function score. Participants in the semaglutide arm experienced improvement from
baseline in SF-36v2 physical functioning score (0.8) compared to placebo which resulted in a
decrease in score (-0.3) (higher is better). Improvement in the IWQOL-Lite-CT physical function
score was higher in the semaglutide arm (4.2) compared to placebo (0.8) (higher is better).
142
See
Table D30 for detailed results.
Liraglutide
The SCALE (Sleep Apnea) trial discussed in the Report also assessed patient-reported outcomes
related to sleep health using two instruments: Epworth Sleepiness Scale (ESS) and Functional
Outcomes of Sleep Questionnaire (FOSQ). For the FOSQ instrument, a higher score indicates less
functional impairment. The ESS assesses daytime sleepiness, with a lower score indicating a lower
propensity for daytime sleepiness. The change from baseline for both the ESS and FOSQ
instruments did not differ significantly between the semaglutide (-2.5 and 1.3, respectively) and
placebo arms (-2.3 and 1.1, respectively) (Table D31).
41,50

©Institute for Clinical and Economic Review, 2022 Page D32
Evidence Report – Medications for Obesity Management Return to Table of Contents
The LOSEIT trial assessed patient-reported outcomes related to knee pain using the KOOS
instrument, with higher scores (scale 0-100) indicating improved disease status (positive is better).
At week 52, participants in the liraglutide arm reported improvement on the KOOS pain instrument
(0.4) compared to placebo arm, which reported a decreased score (-0.6) from baseline.
Additionally, participants in the liraglutide arm reported greater improvement in function in
activities of daily living (1.4) and knee-related quality of life (3.1) compared to those in the placebo
arm (-1.6 and 0.7, respectively). Conversely, change in symptoms had a decreased score in the
liraglutide arm (-1.2) compared to placebo (0.3). Overall, there were no significant differences in
change from baseline score for the KOOS instrument and its subsections observed between the
liraglutide and placebo arms.
143
Phentermine/Topiramate
HRQoL was assessed using the SF-36 instrument, the ESS, and the Pittsburgh Sleep Quality Index in
OB-204. Participants in the phentermine/topiramate group demonstrated greater improvement in
the SF-36 physical functioning subscale compared to placebo.
144,148
Additionally, participants
receiving phentermine/topiramate had a greater improvement compared to participants receiving
placebo in their sleep quality, measured by the ESS (-1.9% vs. -1.8%, respectively), and the PSQI (-
3.1% vs. -0.9%, respectively) (Tables D30 and D31).
Bupropion/Naltrexone
In the Ignite trial, HRQoL was assessed with the IWQOL-Lite total score. Participants receiving the
intervention had a significant improvement in their quality of life (16.4), while participants receiving
usual care slightly decreased in their reported quality of life (-1) (Table D30).
147,149

©Institute for Clinical and Economic Review, 2022 Page D33
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D17. Physical Component HRQoL Outcomes of Key Trials
29-31,34,35,41-45,48,50-52,63-66
Study Name Arms
SF-36v2 Physical
Functioning Score,
Mean Change from
Baseline (SE)
SF-36v2 Physical
Component Score,
Mean Change from
Baseline (SE)
IWQOL-Lite-CT Physical
Function Score, Mean
Change from Baseline
(SE)
Semaglutide
STEP 1
PBO
0.4 (NR)
0.2† (0.3)*
5.3 (NR)
SEM
2.2 (NR)
2.4† (0.2)*
14.7 (NR)
STEP 2
PBO
1† (0.4)
NR
5.3 (1.1)
SEM
2.5† (0.4)
NR
10.1 (1)
STEP 3
PBO
1.6 (NR)
2.3 (NR)
NR
SEM
2.4 (NR)
3 (NR)
NR
Liraglutide
SCALE (Sleep
Apnea)
PBO
NR
1.9 (0.5)
NR
LIR
NR
3 (0.6)
NR
SCALE (Obesity &
Pre-Diabetes)
PBO
NR
2.1 (0.2)*
NR
LIR
NR
3.6 (0.1)*
NR
SCALE (IBT)
PBO
3.8 (NR)
3.8 (0.6)*
14.1 (NR)
LIR
4 (NR)
3.4 (0.6)*
14.9 (NR)
SCALE (Type 2
Diabetes)
PBO
NR
NR
8.9 (1.1)*
LIR
NR
NR
15.2 (0.9)*
SCALE (Insulin)
PBO
2.6 (0.5)*
2.2 (0.5)*
5.7 (NR)
LIR
2.5 (0.6)*
2.7 (0.5)*
8.2 (NR)
Bupropion/Naltrexone
COR-II
PBO
8.2 (0.8)
B/N
14.1 (0.6)
COR-BMOD
PBO
12 (0.8)
B/N
16.5 (0.5)
B/N: bupropion/naltrexone, IWQOL-Lite-CT: Quality of Life-Lite Clinical Trials Version, LIR: liraglutide, NR: not
reported, PBO: placebo, SE: standard error, SEM: semaglutide, SF-36v2: Short Form 36v2 Health Survey
Note: Greyed-out boxes indicate that the HRQoL instrument was not used for any trials within that intervention
group.
*SE manually derived from standard deviation or 95% CIs.
†The number of patients for this outcome may differ from the primary analysis population.

©Institute for Clinical and Economic Review, 2022 Page D34
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D18. Mental Component HRQoL Outcomes of Key Trials
31,35,41,43,48,50,53-66
Study Name Arms
SF-36v2 MCS, Mean Change from
Baseline (SE)
Depression Score, Mean
Change from Baseline (SE)*
Semaglutide
STEP 1
PBO
-2.1‡ (0.3)†
SEM
-1.5‡ (0.2)†
STEP 3
PBO
-2.9 (NR)
SEM
-0.8 (NR)
Liraglutide
SCALE (Sleep Apnea)
PBO
0.9 (0.6)
LIR
1.4 (0.6)
SCALE (Obesity & Pre-
Diabetes)
PBO
-0.9 (0.3)†
LIR
0.2 (0.2)†
SCALE (IBT)
PBO
-2.2 (0.7)†
LIR
-1.2 (0.7)†
SCALE (Insulin)
PBO
-1.7 (0.5)†
LIR
-1.9 (0.6)†
Phentermine/Topiramate
EQUIP
PBO
-1.3 (0.2)†
P/T (low)
-1.2 (0.2)†
P/T (high)
-1.5 (0.1)†
EQUATE
PBO
-0.5 (0.4)†
P/T (low)
-1.3 (0.2)†
P/T (high)
-1.1 (0.4)†
CONQUER
PBO
NR
P/T (low)
NR
P/T (high)
NR
Bupropion/Naltrexone
COR-I
PBO
-0.7 (0.2)
B/N
-0.3‡ (0.2)
COR-II
PBO
-0.5 (0.3)
B/N
-0.3 (0.2)
COR-BMOD
PBO
0‡ (0.4)
B/N
0.1‡ (0.2)
COR-Diabetes
PBO
-1.6 (0.4)
B/N
0 (0.3)
B/N: bupropion/naltrexone, IDS-SR: Inventory of Depressive Symptomology (Self-Report), LIR: liraglutide, MCS:
mental component summary, mg: milligram, NR: not reported, PBO: placebo, PHQ-9: Patient Health
Questionnaire, P/T: phentermine/topiramate, SE: standard error, SEM: semaglutide, SF-36v2: Short Form 36v2
Health Survey
Note: Greyed-out boxes indicate that the HRQoL instrument was not used for any trials within that intervention
group.
*Phentermine/topiramate studies utilized PHQ-9 for depression score, bupropion/naltrexone utilized IDS-SR for
depression score.
†SE manually derived from standard deviation or 95% CIs.
‡The number of patients for this outcome may differ from the primary analysis population.

©Institute for Clinical and Economic Review, 2022 Page D35
Evidence Report – Medications for Obesity Management Return to Table of Contents
Harms
Semaglutide versus Placebo
The most frequent adverse events in the STEP 4 and 6 trials for semaglutide were gastrointestinal-
related symptoms, including nausea, constipation, and diarrhea.
140-142
Beyond gastrointestinal
events, semaglutide appeared relatively well-tolerated. Participants in the semaglutide arms of the
STEP 4 and 6 trials experienced more adverse events (81.3% and 86%, respectively) compared to
those in the placebo arms (75% and 79%, respectively). Similarly for STEP 4, participants in the
semaglutide arm experienced more serious adverse events (SAEs) (7.7%) compared to participants
in the placebo arm (5.6%).
140,141
However, STEP 6 reported a higher rate of serious adverse events
in the placebo arm (7%) compared to the semaglutide arm (5%).
142
One death was reported in each
treatment group for STEP 4, but both were determined to be unrelated to study treatment. There
were no deaths reported in STEP 6. Notable serious adverse events that occurred included one
occurrence of cholecystitis in the STEP 4 intervention arm, five occurrences of cholelithiasis in the
STEP 4 intervention arm (two occurrences in the placebo arm) and two occurrences in the STEP 6
intervention arm, one occurrence of nephrolithiasis in the STEP 4 intervention arm, and one
occurrence of ureterolithiasis in the STEP 4 intervention arm and one occurrence in the STEP 6
intervention arm (one occurrence in the placebo arm). Rates of discontinuation due to adverse
events were higher in the semaglutide arms for both STEP 4 and STEP 6 (2.4% and 3%, respectively)
compared to placebo arm (2.2% and 1%, respectively). Gastrointestinal events were the most
common reported reason for discontinuing due to adverse events. See D19 for detailed harms
results.
Liraglutide versus Placebo
The most common adverse events reported in LOSEIT included gastrointestinal events, with a total
of 264 events in the liraglutide arm versus 144 events in the placebo arm.
143
Participants in the
liraglutide arm experienced more adverse events (96%) compared to those in the placebo arm
(93%). Rates of serious adverse events were similar between both the liraglutide (9%) and placebo
arms (8%) (Table D19). Gastrointestinal serious adverse events occurred in one participant from
the liraglutide arm (ileus leading to surgery) and one participant from the placebo arm
(cholecystitis). There were no deaths reported in the trial. Rates of discontinuation due to adverse
events were higher in the liraglutide arm (10 patients) compared to placebo arm (four patients).
Gastrointestinal events were the most common reported reason for discontinuing due to adverse
events.

©Institute for Clinical and Economic Review, 2022 Page D36
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D19. Harms in Additional Trials of Semaglutide and Liraglutide for the Management of
Obesity
140-143
STEP 4
STEP 6
LOSEIT
Study Arms
Run-in*
PBO†
SEM†
PBO
SEM
PBO
LIR
N
902
268
535
101
199
76
80
Any AE, n (%)
760
(84.3)
201 (75) 435 (81.3) 80 (79) 171 (86) 71 (93) 77 (96)
SAE, n (%)
21 (2.3)
15 (5.6)
41 (7.7)
7 (7)
10 (5)
6 (8)
7 (9)
AEs Leading to
Discontinuation, n (%)
48 (5.3) 6 (2.2) 13 (2.4) 1 (1) 5 (3) 4 (5.3) 10 (12.5)
GI Disorders Leading to
Discontinuation, n (%)
NR NR NR 0 (0) 4 (2) 2 (2.6) 8 (10)
Nausea, n (%)
NR
13 (4.9)
75 (14)
4 (4)
35 (18)
NR
NR
Constipation, n (%)
NR
17 (6.3)
62 (11.6)
3 (3)
52 (26)
NR
NR
Diarrhea, n (%)
NR
19 (7.1)
77 (14.4)
6 (6)
32 (16)
NR
NR
AE: adverse event, GI: gastrointestinal, LIR: liraglutide, n: number, N: total number, NR: not reported, PBO:
placebo, SAE: serious adverse event, SEM: semaglutide
*Timepoint for harms is at Weeks 0-20.
†Timepoint for harms is at Weeks 20-68.
Phentermine/Topiramate versus Placebo
In OB-204, most treatment-emergent adverse events were mild to moderate in severity, and the
incidence of any adverse events was higher in the phentermine/topiramate arm (91%) than in the
placebo arm (78%).
144,148
Adverse reactions that occurred more frequently in the intervention arm
than in the placebo arm included dry mouth (50% vs. 0%), dysgeusia (27% vs. 0%), and sinusitis
(23% vs. 0%). Serious adverse events were rare and were experienced by no participants in the
phentermine/topiramate group, compared to one participant in the placebo group. Over twice
many participants in the intervention arm discontinued due to adverse events (9.1%) compared to
participants in the intervention arm (4.4%). See Table D20 for detailed harms results.
Bupropion/Naltrexone versus Placebo
In CVOT Light, over twice as many participants in the bupropion/naltrexone arm experienced any
adverse events (36%) compared to participants in the placebo arm (15%).
145,146
Rates of serious
adverse events were similar and relatively low across the two arms (9-10%) (Table D20). More
participants in the bupropion/naltrexone arm discontinued due to adverse events (28%) than in the
placebo arm (9%). The most common adverse events that led to discontinuation of the drug in both
the treatment arm and the placebo arm included gastrointestinal adverse reactions (14% and 2%,
respectively), which included nausea, constipation, and vomiting, and central nervous system
reactions (5% and 1%, respectively), which including tremor, dizziness, and headache. Psychiatric
disorders, such as insomnia, anxiety, and depression, leading to discontinuation were infrequently
observed in both arms (3% vs. 1%, respectively).

©Institute for Clinical and Economic Review, 2022 Page D37
Evidence Report – Medications for Obesity Management Return to Table of Contents
In the Ignite trial, serious adverse events during the controlled treatment period (up to 26 weeks)
were low, with one participant in the intervention arm versus zero in the placebo arm experiencing
a serious adverse reaction (Table D20)
147,149
. Through the entire study period at 78 weeks, rates of
serious adverse events were low in both arms, occurring in two patients who continued on
bupropion/naltrexone and zero patients in the placebo arm who switched to the treatment. These
two serious adverse events were considered to be unrelated to the study drug.
At 26 weeks, in the Ignite trial, discontinuations due to adverse events occurred at a higher rate in
the bupropion/naltrexone arm (23%) than in the placebo arm (1.1%).
147,149
Throughout the entire
study period (78 weeks), adverse events that led to discontinuation were observed in 24% of
patients who were randomized to and continued open-label bupropion/naltrexone treatment, and
in 16% of patients who were initially in placebo, but switched to open-label treatment. The most
frequent adverse reactions leading to discontinuation of the treatment for both groups included
nausea (7%), anxiety (2.1%), headache (1.7%), dizziness (1.2%), and insomnia (1.2%). See Table D20
for detailed harms results.

©Institute for Clinical and Economic Review, 2022 Page D38
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D20. Harms in Additional Trials of Phentermine/Topiramate and Bupropion/Naltrexone for
the Management of Obesity and Obesity with Diabetes Mellitus
144-149
OB-204
CVOT Light
Ignite
Study Arms PBO
P/T
(high)
PBO B/N PBO* B/N*
PBO
B/N‡
B/N
B/N‡
N
23
22
4450
4455
89
153
89
153
Any AE, n (%) 18 (78.2) 20 (90.9) 668 (15) 1620 (36.4) 0
27
(17.6)
NR NR
SAE, n (%)
1 (4.4)
0
386 (8.7)
463 (10.4)
0
1 (0.7)
0
2 (1.3)
AE Leading to
Disc., n (%)
1 (4.4) 2 (9.1) 388 (8.7) 1253 (28.1) 1 (1.1)
35
(22.9)
14
(15.7)
37
(24.2)
Gastrointestinal
Disorders
NR NR 84 (1.9)† (2)† NR NR NR NR
Nausea 1 (4.4) 2 (9.1) 21 (0.5)† 333 (7.5)†
16
(10.5)
0 NR NR
Dry Mouth
0
11 (50)
2 (0.04)
21 (0.5)
NR
NR
NR
NR
Nervous System
Disorders
NR NR 52 (1.2)† 226 (5.1)† NR NR NR NR
Headache
NR
NR
14 (0.3)†
51 (1.1)†
2 (1.3)
0
NR
NR
Dizziness
0
1 (4.6)
7 (0.2)†
62 (1.4)†
1 (0.7)
0
NR
NR
Dysgeusia
0
6 (27)
0
16 (0.4)
NR
NR
NR
NR
Infection
NR
NR
NR
NR
NR
NR
NR
NR
Sinusitis
0
5 (23)
0
1 (0.02)
NR
NR
NR
NR
Psychiatric
Disorders
NR NR 39 (0.9)† 136 (3.1)† NR NR NR NR
Anxiety
NR
NR
8 (0.2)†
26 (0.6)†
5 (3.3)
0
NR
NR
Insomnia
NR
NR
16 (0.4)†
35 (0.8)†
2 (1.3)
0
NR
NR
AE: adverse event, B/N: bupropion/naltrexone, disc.: discontinuation, n: number, N: total number, NR: not
reported, PBO: placebo, P/T: phentermine/topiramate, SAE: serious adverse event
*Timepoint up to 26 weeks.
†Rates of AEs leading to discontinuation.
‡Timepoint up to 78 weeks.

©Institute for Clinical and Economic Review, 2022 Page D39
Evidence Report – Medications for Obesity Management Return to Table of Contents
D3. Evidence Tables
Table D21. UPSTF Study Quality
BMI: body mass index, CFB: change from baseline, IBT: intensive behavioral therapy, imp: imputation, ITT: intention to treat, PRO: patient-reported outcome, QoL: quality of life,
T2DM: type 2 diabetes mellitus, USPSTF: United States Preventive Services Task Force
*No publication; the sources for this trial are a conference presentation and ClinicalTrials.gov.
†This was an open-label randomized trial.

©Institute for Clinical and Economic Review, 2022 Page D40
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D22. Study Design
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
Semaglutide
STEP 1
29,32,34,72
Phase III, MC, PBO-
controlled monotherapy
PBO + LI
(n=655)
Counseling
sessions every 4
wks; reduced-
calorie diet and
increase physical
activity; daily diary
to record diet and
exercise
Adults with BMI ≥30
kg/m
2
or ≥27 kg/m
2
with at least 1
weight-related
comorbid condition
DM; uncontrolled
thyroid disease; CVD;
treatment with GLP-1;
5 kg weigh loss within
90 days
129 sites in
16 countries
in Asia,
Europe, and
N/S America
Week 68 & Weeks 68-
120 (for extension trial):
% Δ in body weight,
absolute weight loss,
body weight reduction of
5%, 10%, 15%; waist
circ., SBP, LDL, A1C,
fasting FBG, hsCRP, SF-
36, IWQOL
SC SEM 2.4 mg
+ LI (n=1306)
Extension trial
(Wks 68-120)
-PBO + LI→ Off
treatment
(n=99)
-SC SEM 2.4
mg + LI→ Off
treatment
(n=228)
STEP 2
30
Phase III, MC, PBO-
controlled monotherapy
PBO + LI
(n=403)
Counseling
sessions every 4
wks; reduced-
calorie diet and
increase physical
activity; daily dairy
to record diet and
exercise
Adults with BMI of
≥27 kg/m², HbA1C
of 7-10%, and
diagnosed
with type 2 DM
Uncontrolled thyroid
disease; treatment
with GLP-1;
previous/planned
treatment with
surgery; 5 kg weight
loss within 90 days
149 sites in
12 countries
in Europe,
N/S America,
Middle East,
Africa, and
Asia
Week 68:
% Δ in body weight,
absolute weight loss;
body weight reduction of
5%, 10%, 15%, waist
circ., SBP, LDL, AIC,
fasting FBG, hsCRP, SF-
36, IWQOL, Δ in DM
medication
SC SEM 1.0 mg
+ LI (n=403)
SC SEM 2.4 mg
+ LI (n=404)
STEP 3
31,35,39
PBO + IBT
(n=204)
Low-calorie meal
replacement diet
Adults with BMI ≥30
kg/m
2
or ≥27 kg/m2
41 sites in US Week 68:

©Institute for Clinical and Economic Review, 2022 Page D41
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
Phase III, MC, PBO-
controlled monotherapy
[Nutrisystem] for 8
wks and IBT during
68 wks. IBT:
reduced calorie
diet + physical
activity (100
min/wk increased
by 25 min every 4
wks to reach 200
min/wk) + 30 IBT
visits
with at least 1
weight-related
comorbid condition
DM; prior weight loss
surgery; 5 kg weight
loss within 90 days
% Δ in body weight;
absolute weight loss;
body weight reduction of
5%, 10%, 15%; waist
circ.; SF-36
(68 weeks)
SC SEM 2.4 mg
+ IBT (n=407)
STEP 4
39,140,141
Phase III, MC, PBO-
controlled monotherapy
(Wks 0-20)
Run-in period
(n=803)
Monthly
counseling,
reduced-calorie
diet (500 kcal/d
deficit), increased
physical activity
(150 min/wk),
recorded daily by
participants and
reviewed during
counseling visits
Adults with BMI ≥30
kg/m
2
or ≥27 kg/m
2
with at least 1
weight-related
comorbid condition
HbA1C ≥6.5%; 5 kg
weight loss within 90
days
73 sites in 10
countries in
Europe,
North
America (US),
Middle East
(Israel),
Africa (South
Africa)
Weeks 20-68:
% Δ in body weight;
waist circ., SBP, SF-36
(Wks 20-68)
From run-in
with SEM→
PBO + LI
(n=268)
(Wks 20-68)
From run-in
with SEM→
SC SEM 2.4 mg
+ LI (n=535)
STEP 5
36-38
Phase III, MC, PBO-
controlled monotherapy
PBO + LI (n=
152)
Reduced calorie
diet and increased
physical activity
Adults with BMI ≥30
kg/m
2
or ≥27 kg/m
2
with at least 1
weight-related
comorbid condition
HbA1C ≥6.5%; 5 kg
weight loss within 90
days
41 sites in 5
countries
(North
America,
Europe)
Weeks 52 and 104:
% Δ from baseline in
body weight; body
weight reduction of 10%,
15%; waist circ.; SBP
SC SEM 2.4 mg
+ LI (n=152)
STEP 6
142
PBO + LI
(n=101)
Counseling every 4
wks; reduced
Adults (≥18 in South
Korea, ≥20 in Japan)
5 kg weight loss within
90 days; previous
22 sites in
Japan and 6
Week 68:

©Institute for Clinical and Economic Review, 2022 Page D42
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
Phase III, MC, PBO-
controlled monotherapy
SC SEM 1.7 mg
+ LI (n=101)
caloric intake (500
kcal/d); physical
activity ≥150
min/wk
with BMI ≥35 kg/m
2
with at least 1
weight-related
comorbid condition
OR BMI ≥27 kg/m
2
with 2 or more
weight-related
comorbid
conditions
obesity treatment
with surgery or taking
any medication for
indication of obesity
sites in South
Korea
% Δ from baseline to
week 68 in body weight;
body weight reduction of
10%, 15%; waist circ.;
SBP; A1C
SC SEM 2.4 mg
+ LI (n=199)
Semaglutide vs. Liraglutide
STEP 8
33
Phase III, MC, open-label,
PBO-controlled
monotherapy
PBO +LI (n=85)
Counseling
sessions every 4-6
wks; diet of 500
kcal/d deficit
relative to
baseline; physical
activity ≥150
mins/wk
Adults with BMI ≥30
kg/m
2
or ≥27 kg/m
2
with at least 1
weight-related
comorbid condition
DM, HbA1C ≥6.5%, 5
kg weight loss in last
90 days
19 sites in
the US
Week 68:
% Δ in body weight; body
weight reduction of 10%,
15%, 20%
SC SEM 2.4 mg
+ LI (n=126)
SC LIR 3.0 mg +
LI (n=127)
Liraglutide
SCALE (Maintenance)
40,49
Phase III, MC, PBO-
controlled monotherapy
PBO + LI
(n=210)
Low-calorie diet
run-in with weekly
counseling (4-12
wks) then
counseling weekly
during drug
escalation, then
every 4 wks; 500
kcal/day deficit
relative to
baseline; 150+
min/wk
Lost ≥5% initial
bodyweight during
run-in diet (4-12
wks); adults with
BMI ≥30 kg/m
2
or
≥27 kg/m
2
with
comorbidities of
treated/untreated
dyslipidemia or HTN
Diagnosis, type 1/2
DM; treatment with
GLP-1 or medications
causing significant
weight loss/gain;
bariatric surgery;
history of pancreatitis
36 sites in
the US and
Canada
Week 56:
% Δ body weight; weight
reduction 5%, 10%; waist
circ.; BMI; SBP; LDL;
HbA1C; FPG
SC LIR 3.0 mg +
LI (n=212)
SCALE (Sleep Apnea)
41,50
PBO + LI
(n=179)
Counseling
sessions every 4
Adults 18-64 years;
BMI ≥30 kg/m
2
;
>5% Δ in body weight
during previous 3
Week 32:

©Institute for Clinical and Economic Review, 2022 Page D43
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
Phase III, MC, PBO-
controlled monotherapy SC LIR 3.0 mg +
LI (n=180)
wks; 500 kcal/day
deficit relative to
baseline; 150+
min/wk
moderate-severe
OSA and
unable/unwilling to
use CPAP
months; central sleep
apnea; T1/2 DM
40 sites in
North
America
Δ in AHI; Δ in body
weight; Δ in FPG; Δ in
HbA1C; FOSQ; ESS
SCALE (Type 2
Diabetes)
42,52
Phase III, MC, PBO-
controlled monotherapy
PBO + LI
(n=212)
500 kcal/day
deficit relative to
baseline; 150+
min/wk
Adults ≥18;
overweight or
obese (BMI ≥27
kg/m
2
); T2DM
treated w/ diet and
exercise alone or 1-
3 OHA (metformin,
TZD, sulfonylurea)
≥5 kg weight loss in
last 90 days; previous
surgical treatment;
treatment with GLP-1
or DDP-4 or insulin
within last 3 months
126 sites in 9
countries
(France,
Germany,
Israel, South
Africa, Spain,
Sweden,
Turkey, UK)
Weeks 56:
% Δ body weight; weight
reduction 5%, 10%;
HbA1C; waist circ.
Week 68:
68 weeks: % Δ body
weight; waist circ.
Weeks 56-68:
% Δ body weight; waist
circ.
1.8mg SC LIR +
LI (n=211)
SC LIR 3.0 mg +
LI (n=423)
SCALE (Obesity & Pre-
Diabetes)
43,48
Phase III, MC, PBO-
controlled monotherapy
PBO + LI
(n=1244)
Monthly
counseling; 500
kcal/day deficit
relative to
baseline; 150+
min/wk
Adults ≥18; BMI ≥30
kg/m
2
or ≥27 kg/m
2
with untreated
dyslipidemia/HTN
T1/2 DM; history of
pancreatitis; previous
bariatric surgery
191 sites in
27 countries
(Europe, N/S
America,
Asia, Africa,
Australia)
Week 56:
Weight Δ; weight
reduction 5%, 10%; Δ in
BMI, waist circ., glycemic
control variables
SC LIR 3.0 mg +
LI (n=2487)
SCALE (IBT)
44,51
Phase III, MC, PBO-
controlled monotherapy
PBO + IBT
(n=140)
IBT, comprising
behavioral
counseling,
hypocaloric diet,
physical activity
(100-250 min/wk)
Adults ≥18; BMI ≥30
kg/m
2
≥5 kg weight loss in
last 90 days; T1/2 DM;
use of medications
known to induce
weight loss/gain;
history CVD
17 sites in US
Week 56:
Δ in % body weight;
weight reduction 5%,
10%, 15%; Δ in waist
circ., LDL, SBP, HbA1C;
SC LIR 3.0 mg +
IBT (n=142)

©Institute for Clinical and Economic Review, 2022 Page D44
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
SCALE (Insulin)
45
Phase III, MC, PBO-
controlled monotherapy
PBO + IBT
(n=198)
Hypocaloric diet,
increased physical
activity, behavioral
therapy delivered
in frequent
counseling
sessions
Adults ≥18; BMI ≥27
kg/m
2
; T2DM;
receiving stable
treatment with any
basal insulin and ≤2
OADs
T1DM; ≥5 kg weight
loss in last 90 days;
treatment with GLP-1
or DDP-4 or insulin
within last 3 months;
use of medications
known to induce
significant weight
change in last 90 days
53 sites
globally
Week 56:
% Δ in body weight;
weight reduction 5%,
10%; Δ in waist circ.,
FPG, SBP
SC LIR 3.0 mg +
IBT (n=198)
LOSEIT (KOA)
143
Phase III, single-center,
PBO-controlled
monotherapy
PBO + LI (n=
76)
8 wk lead-in low-
calorie diet (800-
1,000 kcal/day)
with meal
bars/powders and
wkly dietician
consults; 1,200
kcal/day wks 0-8
and 1,500 kcal/day
wks 8-52; dietary
group sessions
every 2 wks in first
8 wks
Adults aged 18-74;
BMI ≥27 kg/m
2
;
symptomatic KOA;
stable body weight
Current use weight
loss/gain medications;
recent/ongoing
participation in
organized weight loss
program; end-stage
KOA on radiography
1 site in the
US
Week 52:
Δ in body weight; HrQoL;
weight reduction 5%,
10%; Δ in BMI, waist circ.
SC LIR 3.0 mg +
LI (n= 80)
Phentermine/Topiramate
EQUIP
56,57
PBO +LI
(n=514)
Provided with
standardized
lifestyle
counseling, (LEARN
Adults 18-70 years,
BMI ≥35 kg/m
2
,
triglycerides ≤200
mg/dl with
Weight gain/loss >5 kg
in 3 months; eating
disorders, bariatric
surgery, glaucoma,
91 sites in
the U.S.
Week 56:
%/kg Δ in body weight;
body weight reduction of
5%, 10%, 15%; waist

©Institute for Clinical and Economic Review, 2022 Page D45
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
Phase III, MC, PBO-
controlled combination
therapy
PT 3.75 mg/23
mg + LI
(n=241)
Manual), advised
to follow 500-kcal
diet deficit,
increase water
consumption,
increase physical
activity
treatment of 0-1
lipid lowering med,
BP ≤140/90 mm Hg
with treatment of
0-2 anti-HTN
medications, and
fasting serum FBG
level ≤110
and nephrolithiasis;
thyroid dysfunction;
current substantial
depression, stroke,
MI, HF, DM
circ.; blood pressure,
heart rate, FBG,
triglycerides, HDL, LDL,
depression
PT 15 mg/92
mg + LI
(n=512)
EQUATE
54,55
Phase III, MC, PBO-
controlled combination
therapy
PBO +LI
(n=109)
LEARN Manual
(Lifestyle, Exercise,
Attitude,
Relationships,
Nutrition,
counseling to
reduce energy
intake by 500
kcal/day, food
diary, increase
physical activity;
brief monthly visits
to discuss progress
Adults 18-70 years
and BMI 30-45
kg/m
2
Use of phentermine or
topiramate within past
3 months, weight
gain/loss of >5 kg, use
of a very low calorie
diet, use of
pharmacotherapy for
weight loss, DM,
stroke, participation in
formal weight loss
program within past 3
months, surgery
34 sites in US
Week 28:
%/kg Δ in body weight;
body weight reduction of
5%, 10%; waist circ.;
blood pressure, heart
rate, FBG, HbA1C,
insulin, inflammatory
biomarkers, concomitant
med use, RBANS,
depression (PHQ-9 & C-
SSRS)
Phentermine
7.5 mg +LI
(n=109)
Topiramate 46
mg +LI (n=108)
PT 7.5 mg/46
mg + LI
(n=107)
Phentermine
15 mg + LI
(n=108)
Topiramate 92
mg +LI (n=107)
PT 15 mg/92
mg + LI
(n=108)

©Institute for Clinical and Economic Review, 2022 Page D46
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
CONQUER
53,58
Phase III, MC, PBO-
controlled combination
therapy
PBO +LI
(n=994)
Provided with
LEARN manual,
advised to
implement
lifestyle changes,
and instructions to
reduce caloric diet
by 500 kcal/day,
monthly check-in
with study staff on
progress
Adults (18-70 years)
with overweight/
obesity, BMI 27-45
kg/m² and 2+
comorbidities: SBP
140-160 mm Hg,
DBP 90-100 mm Hg
(no BMI limit and
diff SBP/DBP
criteria for
diabetic), 2+ anti-
HTN drugs;
concentration of
triglycerides 2.26-
4.52 mmol/L or 2+
lipid-lowering
drugs;
concentration FBG
>5.55 mmol/L,
blood FBG >7.77
mmol/L at 2hr,
T2DM; waist circ.
≥102 cm for men or
≥88 cm for women
Blood pressure
>160/100 mm Hg,
concentration fasting
FBG >13.32 mmol/L or
triglycerides >4.52
mmol/L, T1DM,
antidiabetic drugs
besides metformin,
nephrolithiasis, and
current depressive
symptoms (PHQ 21
total score ≥10),
surgery
93 sites in US
Week 56:
%/kg Δ in body weight;
body weight reduction of
5%, 10%; waist circ.;
BMI, blood pressure,
triglycerides, LDL, HDL,
FBG, insulin, biomarkers,
concomitant drugs,
progression to DM (for
non-diabetic), body
composition
PT 7.5 mg/46
mg + LI
(n=498)
PT 15 mg/92
mg + LI
(n=995)
OB-204
(Winslow 2012)
144,148
PBO + LI (n=23)
Lifestyle
modification
counseling (LEARN
behavioral weight
loss and
Adults 30-65 years,
BMI between 30-40
kg/m
2
, diagnosis of
moderate to severe
Other sleep disorder,
limb movement
arousal index >10,
uncontrolled blood
pressure, unstable
1 site in US
Week 28:
Δ in AHI, OSA
parameters (apnea
index, respiratory
disturbance, oxygen

©Institute for Clinical and Economic Review, 2022 Page D47
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
Phase I/II, single-center
PBO-controlled
combination therapy
PT 15 mg/92
mg + LI (n=22)
management
program)
OSA syndrome, and
AHI ≥15
angina, surgery,
cardiac arrythmia, HF,
valvulopathy, MI
saturation index, arousal
index), PSQI, ESS, SF-36,
change in blood
pressure, heart rate, lipid
profile, glycemic
variables, % Δ weight
loss, body weight
reduction of 5%, 10%
Bupropion/Naltrexone
COR-I
61,62
Phase III, MC, PBO-
controlled combination
therapy
PBO + LI
(n=581)
Hypocaloric diet
(500 kcal
deficit/day),
dietary counseling
and weight
management
booklets, advice
on lifestyle
modification
(instructions,
increase physical
activity)
Adults aged 18-65
years with had BMI
30–45 kg/m² and
uncomplicated
obesity, or BMI 27-
45 kg/m² and
controlled HTN or
dyslipidemia, or
both
DM; vascular, hepatic,
or renal disease;
surgical/device for
obesity; or loss/gain
>4 kg within 3 months,
additional weight loss
drugs
34 sites in US
Week 56:
% Δ in body weight; body
weight reduction of 5%,
10%, 15%; waist circ.;
triglycerides, LDL, HDL,
FBG, insulin, HOMA-IR;
and hsCRP; COEQ; IW-
QOL-Lite; FCI; SBP; DBP;
IDS-SR
BN 360 mg/16
mg + LI
(n=578)
BN 360 mg/32
mg + LI
(n=583)
COR-II
63,64
Phase III, MC, PBO-
controlled combination
therapy
PBO + LI
(n=495)
Instructions to
follow hypocaloric
diet (500 kcal
deficit/day),
increase physical
activity, and
behavioral
modification
Adults aged 18-65
years with had BMI
30-45 kg/m² and
uncomplicated
obesity, or BMI 27-
45 kg/m² and
controlled HTN or
dyslipidemia, or
both
DM; vascular, hepatic,
or renal disease;
surgical/device for
obesity; or loss/gain
>4 kg within 3 months,
additional weight loss
drugs
36 sites in US
Week 56:
%/kg Δ in body weight;
body weight reduction of
5%, 10%, 15%; waist
circ.; triglycerides, LDL,
HDL, FBG, insulin,
HOMA-IR; and hsCRP;
COEQ; IW-QOL-Lite; SBP;
DBP; IDS-SR
BN 360 mg/32
mg + LI
(n=1001)

©Institute for Clinical and Economic Review, 2022 Page D48
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
COR-BMOD
65,66
Phase III, MC, PBO-
controlled combination
therapy
PBO + BMOD
(n=202)
Intensive
behavioral group
modification:
group counseling
(wks 1-16: wkly,
wks 16-28:
biweekly, after wk
28: monthly),
deficit diet (varies
depending on
weight), exercise
gradually
increased to 180
min/wk, diary
entry
Adults 18-65 years
of age, with a BMI
of 30–45 kg/m
2
, or
a BMI of 27-45
kg/m
2
in presence
of controlled HTN
and/or dyslipidemia
DM; sig.
cerebrovascular, CV,
hepatic, or renal
disease; treatment
with bupropion/
naltrexone,
surgical/device
intervention; >4 kg
loss/gain within 3
months
9 sites in US
Week 56:
% Δ in body weight; body
weight reduction of 5%,
10%, 15%; waist circ.;
triglycerides, LDL, HDL,
FBG, insulin, and hsCRP;
IWQOL-Lite; FCI; SBP;
DBP; IDS-SR
BN 360 mg/32
mg + BMOD
(n=591)
COR Diabetes
59,60
Phase III, MC, PBO-
controlled combination
therapy
PBO + LI
(n=159)
Hypocaloric diet
(500 kcal
deficit/day),
dietary counseling
and weight
management
booklets, advice
on behavioral
modification
(instructions,
increase physical
activity [walking at
least 30 min most
days])
Adults aged 18-70
years, with T2DM,
BMI ≥27 and I ≥45
kg/m
2
, HbA1C 7-
10% (53-86
mmol/mol), and
FBG 270 mg/dL
T1DM or “brittle-DM”
or hospitalization/ER
visit due to poor
diabetic control, DM
secondary to
pancreatitis or
pancreatectomy,
loss/gain >5 kg within
3 months, surgical/
device for obesity, tx
with bupropion or
naltrexone, weight
loss program within 1
month, pregnant/
breastfeeding
53 sites in US
Week 56:
% Δ in body weight; body
weight reduction of 5%,
10%; waist circ.;
triglycerides, LDL, HDL,
FBG, insulin, SBP; DBP;
HOMA-IR, hsCRP;
HbA1C; OADs; HbA1C
<7% and <6.5%; rescue
med use for DM; d/c due
to poor glycemic control;
IDS-SR
BN 360 mg/32
mg + LI
(n=265)

©Institute for Clinical and Economic Review, 2022 Page D49
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
CVOT (Light Study)
145,146
Phase IIIb, MC, PBO-
controlled combination
therapy
PBO + LI
(n=4450)
Internet-based
weight
management
program
(resources on
healthy eating,
exercise,
behavioral
modifications,
weekly
lessons/emails),
access to personal
weight loss coach,
program to track
weight, meals,
physical activity,
and low-fat, low-
calorie meal plan
>50 years (women)
or >45 years (men),
BMI between 27-50
kg/m
2
, waist circ. of
>88 cm (women) or
>102 cm (men), and
have characteristics
associated with an
increased risk of
adverse CV
outcomes; and/or
T2DM and at least 2
comorbidities (HTN,
etc.)
MI, angina pectoris,
NYHA class III or IV,
HF, history of stroke,
blood pressure
>145/95 mm Hg,
weight gain/loss of
>3% within 3 months,
bariatric or cardiac
surgery
266 sites in
US
Week 52:
Time from
randomization to first
occurrence of a MACE,
time to first occurrence
of a MACE/
hospitalization for
unstable angina, stroke,
or MI, Δ in body weight,
BMI, waist circ., SBP,
DBP, heart rate
BN 360 mg/32
mg + LI
(n=4455)
Ignite
147,149
Phase IIIb, MC, controlled
combination therapy
Usual care
(including LI)
(n=89)
-CLI: Phone/
internet-based
progressive
nutrition and
exercise program
with
dietician/coach
with individualized
goal setting and
tracking tools
-Usual care: Site-
based LI program,
exercise and
hypocaloric diet
(500 kcal deficit),
Adults age 18-60
years, with either
obesity (BMI 30-45
kg/m
2
) or
overweight (BMI
27-45 kg/m
2
) with
dyslipidemia and/or
controlled HTN
DM; MI within 6
months; angina
pectoris grade
III/IV; clinical history
of strokes, seizures,
cranial trauma,
bulimia, anorexia
nervosa
15 sites in US
Weeks 26* and 78:
%/kg Δ in body weight;
body weight reduction of
5%, 10%, 15%; waist
circ.; triglycerides, LDL,
HDL, FBG, insulin, heart
rate; HOMA-IR; ASEX,
BES Total Score; IWQOL-
Lite; SBP; DBP
BN 360 mg/32
mg + CLI
(n=153)

©Institute for Clinical and Economic Review, 2022 Page D50
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name & Type Intervention(s)
Lifestyle
Intervention
Description
Inclusions Exclusions
Study
Location
Outcomes Available and
Timepoint
nutrition tracker,
pedometer,
literature
AHI: apnea-hypopnea index, A1C: glycated hemoglobin, ASEX: Arizona Sexual Experience Scale, BES: Binge Eating Scale, BMI: body-mass index, BMOD:
behavioral modification, BN: bupropion/naltrexone, BP: blood pressure, cm: centimeter, CLI: comprehensive lifestyle intervention, COEQ: Control of Eating
Questionnaire, CPAP: continuous positive airway pressure, hsCRP: C-reactive protein, C-SSRS: Columbia Suicide Severity Rating Scale, CVD: cardiovascular
disease, d: day, DBP: diastolic blood pressure, dL: deciliter, DM: diabetes mellitus, ER: emergency room, ESS: Epworth Sleepiness Scale, FCI: Food Craving
Inventory, FBG: fasting blood glucose, FOSQ: Functional Outcomes of Sleep Questionnaire, GLP-1: glucagon-like peptide-1, HbA1C: glycated hemoglobin, HDL:
high-density lipoprotein, HOMA-IR: Homeostasis Model Assessment for Insulin Resistance, HRQol: health-related quality of life, HTN: hypertension, IBT:
intensive behavioral therapy, IDS-SR: Inventory of Depressive Symptomatology (Self-Report), IWQOL-Lite: Impact of Weight on Quality of Life-Lite, kcal: calorie,
kg: kilogram, KOA: knee osteoarthritis, L: liter, LDL: low-density lipoprotein, LEARN: lifestyle, exercise, attitudes, relationships, and nutrition, LI: lifestyle
intervention, LIR: liraglutide, m: meter, MACE: major adverse cardiovascular events, MC: multi-center, mg: milligram, min: minute, mmHg: milliliter of mercury,
mmol: millimole, n: number, NYHA: New York Heart Association, OAD: oral antidiabetic drug, OHA: oral hypoglycemic agents, OSA: obstructive sleep apnea,
PBO: placebo, PHQ-9: Patient Health Questionnaire, PSQI: Pittsburgh Sleep Quality Index, PT: phentermine/topiramate, RBANS: Repeatable Battery for the
Assessment of Neuropsychological Status, SBP: systolic blood pressure, SC: subcutaneous, SEM: semaglutide, SF-36: Short Form Health Survey, TZD:
thiazolidinediones, U.K.: United Kingdom, U.S.: United States, vs.: versus
*We focus on the 26-week timepoint, during the randomized period of the trial.

©Institute for Clinical and Economic Review, 2022 Page D51
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D23. Baseline Characteristics I
29-45,48-66,72,140-149
Study Name Intervention(s)
Age, Years
Female
Sex, %
Race/Ethnicity, %
BMI, kg/m
2
Baseline
Weight, kg
Mean
SD
Mean
SD
Mean
SD
Semaglutide
STEP 1
PBO + LI (n=655) 47 12 76
76% White, 12% Asian, 6% Black, 6% other; 13%
Latinx
38 6.5 105.2 21.5
SC SEM 2.4 mg + LI (n=1306) 46 13 73.1
75% White, 14% Asian, 6% Black, 6% other; 12%
Latinx
37.8 6.7 105.4 22.1
STEP 1
(Extension)†
PBO→ Off Treatment (n=99) 50 11 67.7
75% White, 23% Asian, 1% Black, 1% Other; 1%
Hispanic/Latinx
37.7 8 105.4 25.6
SC SEM 2.4 mg + LI→
Off Treatment (n=228)
48 12 66.7
76% White, 19% Asian, 4% Black, <1% Other, 2%
Hispanic/Latinx
37.6 7 105.6 21.8
STEP 2
PBO + LI (n=403) 55 11 47.1
60% White, 27% Asian, 9% Black, 4% other; 12%
Latinx
35.9 6.5 100.5 20.9
SC SEM 1.0 mg + LI (n=403) 56 10 50.4
68% White, 24% Asian, 7% Black, 2% other; 15%
Latinx
35.3 5.9 99 21.1
SC SEM 2.4 mg + LI (n=404) 55 11 55.2
59% White, 28% Asian, 9% Black, 5% other; 12%
Latinx
35.9 6.4 99.9 22.5
STEP 3
PBO + IBT (n=204) 46 13 88.2
78% White, 3% Asian, 18% Black, 2% other; 23%
Latinx
37.8 6.9 103.7 22.9
SC SEM 2.4 mg + IBT (n=407) 46 13 77.4
75% White, 1% Asian, 20% Black, 3% other; 18%
Latinx
38.1 6.7 106.9 22.8
STEP 4
Run-in period (n=803) 46 12 79
84% White, 2% Asian, 13% Black, 1% Other; 8%
LatinX
38.4 6.9 107.2 22.7
From run-in with SEM→
PBO + LI (n=268)*
46 12 76.5
84% White, 2% Asian, 13% Black, 1% Other; 8%
LatinX
34.1 7.1 95.4 22.7
From run-in with SEM→
SC SEM 2.4 mg + LI (n=535)*
47 12 80.2
83% White, 3% Asian, 13% Black, <1% other; 8%
LatinX
34.5 6.9 96.5 22.5
STEP 5
PBO + LI (n=152) 47 10 74.3
93% White, 0% Asian, 3% Black, 1% American
Indian/Alaskan Native, 3% other; 14% Latinx
38.5 6.9 106 NR
SC SEM 2.4 mg + LI (n=152) 47 12 80.9
93% White, 1% Asian, 5% Black, 0% other, 1%
American Indian/Alaskan Native; 12% Latinx
STEP 6
PBO + LI (n=101)
50
9
25.7
100% Asian
31.9
4.2
90.2
15.1
SC SEM 1.7 mg + LI (n=101)
51
10
36.6
100% Asian
31.6
3.7
86.1
11.9
SC SEM 2.4 mg + LI (n=199)
52
12
42.7
100% Asian
32
4.6
86.9
16.5
Semaglutide vs. Liraglutide

©Institute for Clinical and Economic Review, 2022 Page D52
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Intervention(s)
Age, Years
Female
Sex, %
Race/Ethnicity, %
BMI, kg/m
2
Baseline
Weight, kg
Mean
SD
Mean
SD
Mean
SD
STEP 8
PBO + LI (n=85) 51 12 77.6
71% White, 4% Asian, 22% Black, 4% other; 8%
Latinx
38.8 6.5 108.8 23.1
SC SEM 2.4 mg + LI (n=126) 48 14 81
75% White, 3% Asian, 20% Black, 2% other; 12%
Latinx
37 7.4 102.5 25.3
SC LIR 3.0 mg + LI (n=127) 49 13 76.4
75% White, 5% Asian, 16% Black, 5% other; 13%
Latinx
37.2 6.4 103.7 22.5
Liraglutide
SCALE
(Maintenance)
PBO + LI (n=210) 46.5 11 79
88% White, 11% Black, 0% Asian, 0% Native
Hawaiian/Pacific Islander
35.2 5.9 98.7 21.2
SC LIR 3.0 mg + LI (n=212) 45.9 11.9 84
80% White, 15% Black, 1% Asian, 1% Native
Hawaiian/Pacific Islander
36 5.9 100.4 20.8
SCALE
(Sleep Apnea)
PBO + LI (n=179) 48.4 9.5 27.9
75% White, 2% Asian, 20% Black, 1% Native
Hawaiian/Pacific Islander, 2% other; 13% Latinx
39.4 7.4 118.7 25.4
SC LIR 3.0 mg + LI (n=180) 48.6 9.9 28.3
72% White, 7% Asian, 18% Black, 1% Native
Hawaiian/Pacific Islander, 2% other; 11% Latinx
38.9 6.4 116.5 23
SCALE
(Type 2
Diabetes)
PBO + LI (n=212) 54.7 9.8 54.2
83% White, 2% Asian, 13% Black, 2% other; 11%
Latinx
37.4 7.1 106.5 21.3
1.8 mg SC LIR + LI (n=211) 54.9 10.7 48.8
84% White, 2% Asian, 13% Black, 1% other; 8%
Latinx
37 6.9 105.8 21
SC LIR 3.0 mg + LI (n=423) 55 10.8 48
84% White, 3% Asian, 10% Black, 3% other; 11%
Latinx
37.1 6.5 105.7 21.9
SCALE (Obesity
& Pre-
Diabetes)
PBO + LI (n=1244) 45 12 78.1
85% White, 4% Asian, 9% Black, <1% American
Indian/Alaska Native, <1% Native Hawaiian/Pacific
Islander, 1% other; 11% Latinx
38.3 6.3 106.2 21.7
SC LIR 3.0 mg + LI (n=2487) 45.2 12.1 78.7
85% White, 4% Asian, 10% Black, <1% American
Indian/Alaska Native, <1% Native Hawaiian/Pacific
Islander, 2% other; 10% Latinx
38.3 6.4 106.2 21.2
SCALE (IBT)
PBO + IBT (n=140)
49
11.2
82.9
82% White, 2% Asian, 16% Black; 6% Latinx
38.7
7.2
106.7
22
SC LIR 3.0 mg + IBT (n=142)
45.4
11.6
83.8
79% White, 1% Asian, 19% Black; 17% Latinx
39.3
6.8
108.5
22.1
SCALE (Insulin)
PBO + IBT (n=198)
57.6
10.4
50
91% White, 3% Asian, 6% Black; 15% Latinx
35.3
5.8
98.9
19.9
SC LIR 3.0 mg + IBT (n=198)
55.9
11.3
44.5
88% White, 2% Asian, 9% Black; 22% Latinx
35.9
6.5
100.6
20.8
LOSEIT (KOA)
PBO + LI (n=76)
59.3
9.7
64
NR
31.3
4
90.8
14.3
SC LIR 3.0 mg + LI (n=80) 59.2 10.8 65 NR 32.8 5.5 96.3 18.2

©Institute for Clinical and Economic Review, 2022 Page D53
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Intervention(s)
Age, Years
Female
Sex, %
Race/Ethnicity, %
BMI, kg/m
2
Baseline
Weight, kg
Mean
SD
Mean
SD
Mean
SD
Phentermine/Topiramate
EQUIP
PBO + LI (n=514) 43 11.8 82.7
80% White, 18% Black, 1% American Indian/Alaskan
Native, <1% Asian, <1% Native Hawaiian/Pacific
Islander, <1% other
42 6.2 115.8 21.5
P/T 3.75 mg/23 mg + LI
(n=241)
43 11 83.4
80% White, 16% Black, <1% American
Indian/Alaskan Native, <1% Asian, <1% Native
Hawaiian/Pacific Islander, 2% other
42.6 6.5 118.5 21.9
P/T 15 mg/92 mg + LI (n=512) 41.9 12.2 82.8
80% White, 18% Black, 1% American Indian/Alaskan
Native, <1% Asian, <1% Native Hawaiian/Pacific
Islander, 1% other
41.9 6 115.2 20.7
EQUATE
PBO + LI (n=109)
45
11.4
78.9
76% White, 23% Black, 0% Asian, 1% other
36.2
3.9
100
13
Phentermine 7.5 mg + LI
(n=109)
46.4 11.6 78.9 74% White, 24% Black, 2% Asian, 2% other 36.3 4 101 15.1
Topiramate 46 mg + LI (n=108)
46.9
12.6
79.6
88% White, 10% Black, 2% Asian, 2% other
36.1
4.1
100.7
16.3
P/T 7.5 mg/46 mg + LI (n=107)
44.6
11.1
79.4
75% White, 24% Black, 0% Asian, 1% other
36.6
3.9
102.2
16.5
Phentermine 15 mg + LI
(n=108)
45.7 12.4 79.6 83% White, 13% Black, 1% Asian, 3% other 36.2 4.2 101.4 16.4
Topiramate 92 mg +LI (n=107)
45.8
11.2
79.4
77% White, 21% Black, 2% Asian, 2% other
37
4.3
104.5
15.6
P/T 15 mg/92 mg + LI (n=108)
44.6
12.8
78.7
82% White, 15% Black, 2% Asian, 3% other
35.9
3.9
99.3
15.6
CONQUER
(Diabetes
subgroup)
PBO +LI (n=157) 52.6 9.8 71.3
85% White, 12% Black, 2% Asian, 2% other
29% Hispanic/Latinx, 71% not Hispanic/Latinx
36.2 5.2 99.3 18.6
P/T 7.5 mg/46 mg + LI (n=67) 52.5 9.3 65.6
94% White, 5% Black, 0% Asian, 2% other
31% Hispanic/Latinx, 69% not Hispanic/Latinx
35.3 4.3 97.2 16.1
P/T 15 mg/92 mg + LI (n=164) 52.1 10.1 62.1
83% White, 14% Black, 2% Asian, 3% other
31% Hispanic/Latinx, 69% not Hispanic/Latinx
37.1 5.2 103.2 20.1
OB-204
(Winslow
2012)
PBO + LI (n=23) 51.4 5.7 34.8
91% White, 9% Black, 4% Hispanic/Latinx, 96% not
Hispanic/Latinx
35.3 3.1 106.9 16.7
P/T 15 mg/92 mg + LI (n=22) 53.4 7 59.1
91% White, 9% Black, 0% Hispanic/Latinx, 100% not
Hispanic/Latinx
36 3.1 103.7 14.6
Bupropion/Naltrexone
COR-I
PBO + LI (n=581)
43.7
11.1
85
76% White, 19% Black, 5% other
36.2
4
99.5
14.3
B/N 360 mg/16 mg + LI
(n=578)
44.4 11.3 85 74% White, 21% Black, 5% other 36.2 4.3 99.5 14.8
B/N 360 mg/32 mg + LI
(n=583)
44.4 11.1 85 75% White, 18% Black, 6% other 36.1 4.4 99.7 15.9

©Institute for Clinical and Economic Review, 2022 Page D54
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Intervention(s)
Age, Years
Female
Sex, %
Race/Ethnicity, %
BMI, kg/m
2
Baseline
Weight, kg
Mean
SD
Mean
SD
Mean
SD
COR-II
PBO + LI (n=495)
44.4
11.4
84.8
84% White, 15% Black, 2% other
36.1
4.3
99.2
15.9
B/N 360 mg/32 mg + LI
(n=1001)
44.3 11.2 84.6 83% White, 13% Black, 3% other 36.2 4.5 100.3 16.6
COR-BMOD
PBO + BMOD (n=202)
45.6
11.4
91.6
74% White, 22% African American, 5% other
37
4.2
101.9
15
B/N 360 mg/32 mg + BMOD
(n=591)
45.9 10.4 89.3 69% White, 25% African American, 7% other 36.3 4.2 100.2 15.4
COR Diabetes
PBO + LI (n=159)
53.8
9.7
52.8
83% White, 11% Black, 6% other
36.3
4.5
105
17.1
B/N 360 mg/32 mg + LI
(n=265)
53.9 9.2 54.3 78% White, 19% Black, 3% other 36.7 4.8 106.3 19.1
CVOT (Light
Study)
PBO + LI (n=4450) 60.9 7.4 54.4
83% White, 15% Black/African American, <1% Asian,
<1% American Indian/Alaskan Native, <1% Native
Hawaiian/Pacific Islander
93% non-Hispanic/Latinx, 7% Hispanic/Latinx
37.4 5.4 106.3 19.2
B/N 360 mg/32 mg + LI
(n=4455)
61.1 7.3 54.7
84% White, 15% Black/African American, <1% Asian,
<1% American Indian/Alaskan Native, <1% Native
Hawaiian/Pacific Islander
94% non-Hispanic/Latinx, 6% Hispanic/Latinx
37.2 5.3 105.6 19.1
Ignite
Usual care (including LI) (n=89) 47 10 86.5
72% White, 27% Black/African American, 0% Asian,
1% American Indian/Alaskan Native
6% Hispanic/LatinX, 94% not Hispanic/Latinx
36.3 4.4 100.2 16.6
B/N 360 mg/32 mg + CLI
(n=153)
46.1 9.7 81.7
81% White, 18% Black/African American, 1% Asian,
0% American Indian/Alaskan Native
3% Hispanic/LatinX, 97% not Hispanic/Latinx
36.3 4.2 101.4 15.1
BMI: body-mass index, BMOD: behavioral modification, B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, IBT: intensive behavioral therapy, kg:
kilogram, KOA: knee osteoarthritis, LI: lifestyle intervention, LIR: liraglutide, m: meter, mg: milligram, n: number, NR: not reported, PBO: placebo, P/T:
phentermine/topiramate, SC: subcutaneous, SD: standard deviation, SEM: semaglutide, vs.: versus
*Baseline data measured at Week 20.
†Baseline data measured at Week 68.

©Institute for Clinical and Economic Review, 2022 Page D55
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D24. Baseline Characteristics II
29-45,48-66,72,140-149
Study Name Intervention(s)
Waist
Circumference,
cm
A1C, Mean %
Diabetes
%
Pre-
Diabetes,
%
SBP, mm HG LDL, mg/dL
Fasting Blood
Glucose,
mg/dL
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Semaglutide
STEP 1
PBO + LI (n=655)
114.8
14.4
5.7
0.3
0
40.2
127
14
112.5
29.8
94.7
10.5
SC SEM 2.4 mg + LI
(n=1306)
114.6 14.8 5.7 0.3 0 45.4 126 14 110.3 31.6 95.4 10.7
STEP 1
(Extension)#
PBO→ Off Treatment
(n=99)
NR NR 5.7 0.3 0 53.5 130 15 113.7 NR NR NR
SC SEM 2.4 mg + LI→
Off Treatment
(n=228)
NR NR 5.7 0.3 0 62.3 129 14 113.4 29.4 NR NR
STEP 2
PBO + LI (n=403)
115.5
13.9
8.1
0.8
100
0
130
13
89*
NR
158.4*
41.4
SC SEM 1.0 mg + LI
(n=403)
113.9 14 8.1 0.8 100 0 130 14 89* NR 154.8* 41.4
SC SEM 2.4 mg + LI
(n=404)
114.5 14.3 8.1 0.8 100 0 130 13 89* NR 153* 41.4
STEP 3
PBO + IBT (n=204)
111.8
16.2
5.8
0.3
0
52.9
124
15
111.8*
31.2
94*
9.8
SC SEM 2.4 mg + IBT
(n=407)
113.6 15.1 5.7 0.3 0 48.2 124 15 107.7* 30.3 93.9* 9.4
STEP 4
Run-in period (n=803) 115.3 15.5 5.7 0.3 0 NR 127 14 116.6*
IQR:
97.3-
138.6
97 10.7
From run-in with
SEM→ PBO + LI
(n=268)§
104.7 16.9 5.4 0.3 0 42.5 121 13 112.5
IQR:
93.6-
130.9
86.9 7.6
From run-in with
SEM→ SC SEM 2.4 mg
+ LI (n=535)§
105.5 15.9 5.4 0.3 0 49 121 13 110.4
IQR:
91.1-
130.9
87.9 7.7
STEP 5
PBO + LI (n=152)
115.7 14.8 5.7 0.3
0
46.4 125.5 14.5 112.1 NR 95.4 10.8
SC SEM 2.4 mg + LI
(n=152)
0
STEP 6
PBO + LI (n=101)
103.8
9.9
6.4
1.1
25
25
133
14
123.7
NR
113.5
28.8

©Institute for Clinical and Economic Review, 2022 Page D56
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Intervention(s)
Waist
Circumference,
cm
A1C, Mean %
Diabetes
%
Pre-
Diabetes,
%
SBP, mm HG LDL, mg/dL
Fasting Blood
Glucose,
mg/dL
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Mean
SD
SC SEM 1.7 mg + LI
(n=101)
101.4 8.8 6.4 1.1 25 21 135 13 119.9 NR 111.7 27
SC SEM 2.4 mg + LI
(n=199)
103.8 11.8 6.4 1.2 25 22 133 14 116 NR 111.7 27
Semaglutide vs. Liraglutide
STEP 8
PBO + LI (n=85)
115.4
15.1
5.6
0.4
0
40
123
14
105.2
NR
97.6
12.2
SC SEM 2.4 mg + LI
(n=126)
111.8 16.3 5.5 0.3 0 34.1 125 14 106.4 NR 96.1 10.2
SC LIR 3.0 mg + LI
(n=127)
113.5 15 5.5 0.3 0 35.4 126 16 108.1 NR 95.2 8.5
Liraglutide
SCALE
(Maintenance)
PBO + LI (n=210)
107.8
15.2
5.6
0.4
0
NR
117.8
10.8
104.4
30.9
99
10.8
SC LIR 3.0 mg + LI
(n=212)
109.4 15.3 5.6 0.4 0 NR 116.6 12.5 100.5 27.1 97.2 9
SCALE (Sleep
Apnea)
PBO + LI (n=179)
122.7
14.9
5.6
0.4
0
62.6
127.1
12.3
111.4
26.8
97.2
16.2
SC LIR 3.0 mg + LI
(n=180)
122.3 14.5 5.7 0.4 0 63.9 125.8 11.5 111.6 28.9 97.2 10.8
SCALE (Type 2
Diabetes)
PBO + LI (n=212)
117.3
14
7.9
0.8
100
0
129.2
13.6
85.2
39.3
155.5
33
1.8 mg SC LIR + LI
(n=211)
117.5 14.7 8 0.8 100 0 130.5 14.5 91.5 38.5 160.4 35.1
SC LIR 3.0 mg + LI
(n=423)
118 14.4 7.9 0.8 100 0 128.9 13.6 86.4 35.5 158.4 32.8
SCALE (Obesity
& Pre-
Diabetes)
PBO + LI (n=1244)
114.5
14.3
5.6
0.4
0
60.9
123.2
12.8
112.2
27.6
95.5
9.8
SC LIR 3.0 mg + LI
(n=2,487)
115 14.4 5.6 0.4 0 61.4 123 12.9 111.6 27.9 95.9 10.6
SCALE (IBT)
PBO + IBT (n=140)
115
15.6
5.5
0.4
0
NR
127
14
119.9
34.8
97.2
10.5
SC LIR 3.0 mg + IBT
(n=142)
116 14.4 5.5 0.4 0 NR 125 15 112.1 30.9 97.2 9
SCALE (Insulin)
PBO + IBT (n=198)
114.2
13.2
8
1
100
0
132
16
94
29
164
46
SC LIR 3.0 mg + IBT
(n=198)
114.8 13.7 7.9 1.1 100 0 129 14 94 33 141 40
LOSEIT (KOA)
PBO + LI (n=76)
101.8
11.1
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR

©Institute for Clinical and Economic Review, 2022 Page D57
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Intervention(s)
Waist
Circumference,
cm
A1C, Mean %
Diabetes
%
Pre-
Diabetes,
%
SBP, mm HG LDL, mg/dL
Fasting Blood
Glucose,
mg/dL
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Mean
SD
SC LIR 3.0 mg + LI
(n=80)
105.5 13.9 NR NR NR NR NR NR NR NR NR NR
Phentermine/Topiramate
EQUIP
PBO +LI (n=514)
120.5
13.9
NR
NR
0
NR
121.8
11.5
121.3
32
93
8.7
P/T 3.75 mg/23 mg +
LI (n=241)
121.7 15.2 NR NR 0 NR 122.5 11.1 122.5 33 93.8 9.11
P/T 15 mg/92 mg + LI
(n=512)
120.1 14.6 NR NR 0 NR 122 11.6 119.8 30.1 93 9.47
EQUATE
PBO +LI (n=109)
110.7
9.5
5.4*
0.41
0
NR
120.6
14.1
NR
NR
5.3*
0.59
Phentermine 7.5 mg
+LI (n=109)
111.7 10.8 5.5* 0.4 0 NR 122.3 12.9 NR NR 5.2* 0.53
Topiramate 46 mg +
LI (n=108)
110.6 11.5 5.5* 0.43 0 NR 123.4 13.7 NR NR 5.2* 0.55
P/T 7.5 mg/46 mg + LI
(n=107)
111.7 12.9 5.4* 0.42 0 NR 123.4 12.2 NR NR 5.2* 0.55
Phentermine 15 mg +
LI (n=108)
111.2 11.3 5.4* 0.37 0 NR 120.5 13.4 NR NR 5.2* 0.53
Topiramate 92 mg +
LI (n=107)
112.6 11.3 5.5* 0.38 0 NR 123.2 14.1 NR NR 5.3* 0.5
P/T 15 mg/92 mg + LI
(n=108)
109.5 10.5 5.5* 0.43 0 NR 121.2 12.4 NR NR 5.3* 0.55
CONQUER
(Diabetes
Subgroup)
PBO + LI (n=157)
112.7
12.5
6.9
1.3
100
NR
125.7
13.9
3
0.9
NR
NR
P/T 7.5 mg/46 mg + LI
(n=67)
111.4 10.8 6.8 1.2 100 NR 127 12.1 2.8 0.9 NR NR
P/T 15 mg/92 mg + LI
(n=164)
114.1 12.8 6.8 1.1 100 NR 126 14 3 1 NR NR
OB-204
(Winslow
2012)
PBO + LI (n=23)
NR
NR
NR
NR
NR
NR
138.4
13.5
121.5
36.2
109.2
46.6
P/T 15 mg/92 mg + LI
(n=22)
NR NR NR NR NR NR 137.5 12.1 131.6 35.5 110.2 30.1
Bupropion/Naltrexone
COR-I
PBO + LI (n=581)
110
12.2
NR
NR
0
NR
119
9.8
3.1
0.9
93.6
10.8
B/N 360 mg/16 mg +
LI (n=578)
109.8 11.2 NR NR 0 NR 119.5 9.9 3.2 0.8 95.4 10.8

©Institute for Clinical and Economic Review, 2022 Page D58
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Intervention(s)
Waist
Circumference,
cm
A1C, Mean %
Diabetes
%
Pre-
Diabetes,
%
SBP, mm HG LDL, mg/dL
Fasting Blood
Glucose,
mg/dL
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Mean
SD
B/N 360 mg/32 mg +
LI (n=583)
108.8 11.3 NR NR 0 NR 118.9 9.9 3.1 0.8 93.6 12.6
COR-II
PBO + LI (n=495)
108.9*
11.7
NR
NR
0
NR
118.2*
10.5
117.1*
32.6
94.2*
10.4
B/N 360 mg/32 mg +
LI (n=1,001)
109.3* 11.9 NR NR 0 NR 118.1* 10 119.8* 30.2 94.8* 11.2
COR-BMOD
PBO + BMOD (n=202)
109
11.8
NR
NR
0
NR
116.7
10.9
109.2
27.3
94.1
20.1
B/N 360 mg/32 mg +
BMOD (n=591)
109.3 11.4 NR NR 0 NR 116.6 10.1 109.5 27.5 92.4 10.7
COR Diabetes
PBO + LI (n=159)
114.3
12.4
8
0.9
100
NR
124.5
9.6
101
33.9
163.9
44.5
B/N 360 mg/32 mg +
LI (n=265)
115.6 12.6 8 0.8 100 NR 125 11 100.2 34.2 160 41.3
CVOT (Light
Study)
PBO + LI (n=4,450) 118.5†
IQR:
110-
128
7.1‡
IQR:
6.4-
8.2
85.5 NR 125.5 12.6 82†
IQR:
65-
106
NR NR
B/N 360 mg/32 mg +
LI (n=4,455)
118†
IQR:
110-
128
7‡
IQR:
6.1-
8.1
84.9 NR 125.9 12.5 82†
IQR:
64-
105
NR NR
Ignite
Usual care (including
LI) (n=89)
111.9 11.9 NR NR 0 NR 120.6 11.4 118* 26.2 92.4* 11.5
B/N 360 mg/32 mg +
CLI (n=153)
112.2 11.2 NR NR 0 NR 123.7 9.5 115.5* 27.6 89.7* 10.6
A1C: glycated hemoglobin, BMOD: behavioral modification, B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, cm: centimeter, dL: deciliter,
IBT: intensive behavioral therapy, IQR: interquartile range, KOA: knee osteoarthritis, LDL: low-density lipoprotein, LI: lifestyle intervention, LIR: liraglutide, mg:
milligram, mm Hg: millimeter of mercury, n: number, NR: not reported, PBO: placebo, P/T: phentermine/topiramate, SBP: systolic blood pressure, SC:
subcutaneous, SD: standard deviation, SEM: semaglutide, vs.: versus
*The number of patients for this characteristic may differ from the randomized population.
†Median.
‡Measured only in patients who had diabetes mellitus.
§Baseline data measured at Week 20.
#Baseline data measured at Week 68.

©Institute for Clinical and Economic Review, 2022 Page D59
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D25. Baseline Characteristics III
29-35,39-43,45,48-50,52-66,72,140-142,145,146
Study Name
Intervention(s)
Pre-Existing Conditions
Medications
Semaglutide
STEP 1
PBO + LI (n=655)
Dyslipidemia (35%), HTN (36%), knee arthritis (16%),
sleep apnea (11%), asthma/COPD (12%), NAFLD (10%),
PCOS (7%), CAD (3%)
Antihypertensive; lipid lowering
SC SEM 2.4 mg + LI
(n=1306)
Dyslipidemia (38%), HTN (36%), knee arthritis (13%),
sleep apnea (12%), asthma/COPD (11%), NAFLD (7%),
PCOS (7%), CAD (3%)
STEP 1
(Extension)†
PBO→ Off Treatment
(n=99)
Dyslipidemia (40%), HTN (38%), KOA (19%), OSA (10%),
asthma/COPD (10%), NAFLD (16%), PCOS (10%), CAD
(2%)
GLP-1 (4%)
SC SEM 2.4 mg + LI→
Off Treatment
(n=228)
Dyslipidemia (42%), HTN (40%), KOA (11%), OSA (8%),
asthma/COPD (16%), NAFLD (9%), PCOS (13%), CAD (3%)
GLP-1 (6%)
STEP 2
PBO + LI (n=403)
CAD (8%), Dyslipidemia (71%), HTN (71%), knee arthritis
(17%), OSP (13%), NAFLD (23%), PCOS (5%),
asthma/COPD (8%)
Biguaindes (90%), Sulfonylureas (25%), SGLT2i
(26%), TZDs (5%), DDP4i (<1%), GLP-1 (<1%)
SC SEM 1.0 mg + LI
(n=403)
CAD (10%), Dyslipidemia (71%), HTN (71%), knee
arthritis (14%), OSP (13%), NAFLD (20%), PCOS (4%),
asthma/COPD (12%)
Biguaindes (94%), Sulfonylureas (25%), SGLT2i
(24%), TZDs (4%), DDP4i (<1%), GLP-1 (<1%)
SC SEM 2.4 mg + LI
(n=404)
CAD (6%), Dyslipidemia (66%), HTN (68%), knee arthritis
(18%), OSP (17%), NAFLD (21%), PCOS (3%),
asthma/COPD (9%)
Biguaindes (92%), Sulfonylureas (27%), SGLT2i
(25%), TZDs (5%), DDP4i (<1%), GLP-1 (<1%)
STEP 3
PBO + IBT (n=204)
Dyslipidemia (33%), HTN (33%), knee arthritis (15%),
asthma/COPD (12%), OSP (9%), NAFLD (6%), PCOS (6%),
CAD (2%)
NR
SC SEM 2.4 mg + IBT
(n=407)
Dyslipidemia (36%), HTN (36%), knee arthritis (19%),
asthma/COPD (17%), OSP (14%), NAFLD (6%), PCOS
(5%), CAD (2%)
NR
STEP 4
Run-in period (n=803)
Dyslipidemia (36%), HTN (37%), knee arthritis (12%),
OSA (12%), asthma/COPD (12%), NAFLD (7%), PCOS
(4%), CAD (<1%)
NR
From run-in with
SEM→ PBO + LI
(n=268)*
Dyslipidemia (37%), HTN (37%), knee arthritis (10%),
OSA (12%), asthma/COPD (13%), NAFLD (7%), PCOS
(5%), CAD (1%)
NR

©Institute for Clinical and Economic Review, 2022 Page D60
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name
Intervention(s)
Pre-Existing Conditions
Medications
From run-in with
SEM→ SC SEM 2.4 mg
+ LI (n=535)*
Dyslipidemia (35%), HTN (37%), knee arthritis (14%),
OSA (11%), asthma/COPD (11%), NAFLD (7%), PCOS
(4%), CAD (<1%)
NR
STEP 5
PBO + LI (n=152)
NR
NR
SC SEM 2.4 mg + LI
(n=152)
NR NR
STEP 6
PBO + LI (n=101)
Dyslipidemia (79%), HTN (72%), NAFLD (46%), kidney
disease (13%), OSA (10%), knee arthritis (9%)
Biguanides (72%), SGLT2 inhibitors (52%),
Sulfonylureas (32%), Thiazolidinediones (12%)
SC SEM 1.7 mg + LI
(n=101)
Dyslipidemia (87%), HTN (73%), NAFLD (40%), kidney
disease (15%), OSP (13%), knee arthritis (9%)
Biguanides (60%), SGLT2 inhibitors (44%),
Sulfonylureas (24%), Thiazolidinediones (16%)
SC SEM 2.4 mg + LI
(n=199)
Dyslipidemia (90%), HTN (76%), NAFLD (47%), kidney
disease (14%), OSP (9%), knee arthritis (11%)
Biguanides (53%), SGLT2 inhibitors (41%),
Sulfonylureas (14%), Thiazolidinediones (16%)
Semaglutide vs. Liraglutide
STEP 8
PBO +LI (n=85)
Dyslipidemia (42%), HTN (46%), knee arthritis (26%),
OSA (22%), asthma/copd (15%), NAFLD (8%), PCOS (2%),
CAD (5%)
NR
SC 2.4 mg + LI (n=126)
Dyslipidemia (48%), HTN (38%), knee arthritis (18%),
OSA (19%), asthma/copd (14%), NAFLD (4%), PCOS (5%),
CAD (3%)
NR
SC LIR 3.0 mg + LI
(n=127)
Dyslipidemia (51%), HTN (43%), knee arthritis (13%),
OSA (14%), asthma/copd (14%), NAFLD (9%), PCOS (6%),
CAD (2%)
NR
Liraglutide
SCALE
(Maintenance)
PBO + LI (n=210)
Dyslipidemia (31%), HTN (29%)
NR
SC LIR 3.0 mg + LI
(n=212)
Dyslipidemia (28%), HTN (33%) NR
SCALE (Sleep
Apnea)
PBO + LI (n=179)
Dyslipidemia (31%), HTN (43%)
SC LIR 3.0 mg + LI
(n=180)
Dyslipidemia (36%), HTN (42%)
SCALE (Type 2
Diabetes)
PBO + LI (n=212)
Dyslipidemia (59%), HTN (68%)
Metformin, glitazone, sulfonylurea
1.8mg SC LIR + LI
(n=211)
Dyslipidemia (68%), HTN (70%)
SC LIR 3.0 mg + LI
(n=423)
Dyslipidemia (70%), HTN (69%)
PBO + LI (n=1244)
Dyslipidemia (29%), HTN (36%)
Anti-hypertensives (33%), lipid-lowering drugs (15%)

©Institute for Clinical and Economic Review, 2022 Page D61
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name
Intervention(s)
Pre-Existing Conditions
Medications
SCALE (Obesity
& Pre-Diabetes)
SC LIR 3.0 mg + LI
(n=2487)
Dyslipidemia (39%), HTN (34%) Anti-hypertensives (31%), lipid-lowering drugs (16%)
SCALE (IBT)
PBO + IBT (n=140)
NR
NR
SC LIR 3.0 mg + IBT
(n=142)
NR NR
SCALE (Insulin)
PBO + IBT (n=198)
NR
biguanides, sulfonylureas, SGLT2i, TZDs
SC LIR 3.0 mg + IBT
(n=198)
NR
LOSEIT (KOA)
PBO + LI (n=76)
NR
NR
SC LIR 3.0 mg + LI
(n=80)
NR NR
EQUIP
PBO +LI (n=514)
Depression (16%)
Antidepressants (13%)
P/T 3.75 mg/23 mg +
LI (n=241)
Depression (20%) Antidepressants (15%)
P/T 15 mg/92 mg + LI
(n=512)
Depression (15%) Antidepressants (13%)
EQUATE
PBO + LI (n=109)
HTN (33%) & dyslipidemia (22%)
SSRIs (9%)
Phentermine 7.5 mg +
LI (n=109)
HTN (32%) & dyslipidemia (26%) SSRIs (13%)
Topiramate 46 mg +
LI (n=108)
HTN (23%) & dyslipidemia (31%) SSRIs (13%)
P/T 7.5 mg/46 mg + LI
(n=107)
HTN (24%) & dyslipidemia (17%) SSRIs (12%)
Phentermine 15 mg +
LI (n=108)
HTN (34%) & dyslipidemia (35%) SSRIs (13%)
Topiramate 92 mg +
LI (n=107)
HTN (27%) & dyslipidemia (27%) SSRIs (10%)
P/T 15 mg/92 mg + LI
(n=108)
HTN (30%) & dyslipidemia (24%) SSRIs (10%)
CONQUER
(Diabetes
Subgroup)
PBO +LI (n=157)
Dyslipidemia (32%) & HTN (52%)
NR
P/T 7.5 mg/46 mg + LI
(n=67)
Dyslipidemia (40%) & HTN (60%) NR
P/T 15 mg/92 mg + LI
(n=164)
Dyslipidemia (32%) & HTN (55%) NR
PBO + LI (n=23)
NR
NR

©Institute for Clinical and Economic Review, 2022 Page D62
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name
Intervention(s)
Pre-Existing Conditions
Medications
OB-204
(Winslow 2012)
P/T 15 mg/92 mg + LI
(n=22)
NR NR
COR-I
PBO + LI (n=581)
HTN (19%) and dyslipidemia (50%)
NR
B/N 360 mg/16 mg +
LI (n=578)
HTN (20%) and dyslipidemia (50%) NR
B/N 360 mg/32 mg +
LI (n=583)
HTN (22%) and dyslipidemia (49%) NR
COR-II
PBO + LI (n=495)
HTN (21%) and dyslipidemia (53%)
NR
B/N 360 mg/32 mg +
LI (n=1001)
HTN (21%) and dyslipidemia (56%) NR
COR-BMOD
PBO + BMOD (n=202)
HTN (NR) and dyslipidemia (NR) NR
B/N 360 mg/32 mg +
BMOD (n=591)
COR Diabetes
PBO + LI (n=159)
Dyslipidemia (86%)
Sulfonylurea (49%), TZDs (31%), Metformin (77%)
B/N 360 mg/32 mg +
LI (n=265)
Dyslipidemia (83%) Sulfonylurea (49%), TZDs (31%), Metformin (80%)
CVOT (Light
Study)
PBO + LI (n=4450)
CVD (33%), diabetes (86%), CVD & diabetes (18%), HTN
(93%), dyslipidemia (92%)
Statin (79%), Insulin (23%), Metformin (57%), B-
Blocker (38%), Diuretic (32%), ACE inhibitor/ARB
(77%), Calcium channel blocker (19%)
B/N 360 mg/32 mg +
LI (n=4455)
CVD (32%), diabetes (85%), CVD & diabetes (17%), HTN
(93%), dyslipidemia (92%)
Statin (79%), Insulin (23%), Metformin (57%), B-
Blocker (40%), Diuretic (33%), ACE inhibitor/ARB
(77%), Calcium channel blocker (20%)
Ignite
Usual care (including
LI) (n=89)
NR NR
B/N 360 mg/32 mg +
CLI (n=153)
NR NR
ACE: angiotensin-converting enzyme, ARB: angiotensin II receptor blocker, BMOD: behavioral modification, B/N: bupropion/naltrexone, CAD: coronary artery
disease, CLI: comprehensive lifestyle intervention, COPD: chronic obstructive pulmonary disease, CVD: cardiovascular disease, DDp4i:
dipeptidyl peptidase-4,
GLP-1:
glucagon-like peptide-1, HTN: hypertension, IBT: intensive behavioral therapy, KOA: knee osteoarthritis, LI: lifestyle intervention, LIR: liraglutide, mg:
milligram, n: number, NAFLD: nonalcoholic fatty liver disease, NR: not reported, OSA: obstructive sleep apnea, OSP: oral sodium phosphate, PBO: placebo,
PCOS: polycystic ovarian syndrome, P/T: phentermine/topiramate, SC: subcutaneous, SEM: semaglutide, SGLT2: sodium-glucose cotransporter-2, TZD:
thiazolidinediones, vs.: versus
*Baseline data measured at Week 20.
†Baseline data measured at Week 68.

©Institute for Clinical and Economic Review, 2022 Page D63
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D26. Efficacy: Weight Loss Outcomes I
29-38,40-45,48-67,72,140-149
Study Name Arms N
Change in Body Weight from
Baseline, Mean kg
Weight Loss from Baseline
to Six Months, Mean %
Weight Loss from Baseline
to One Year, Mean %
N
Mean
SE
N
Mean
SE
N
Mean
SE
Semaglutide
STEP 1
PBO + LI
655
577
-2.6
NR
592
-2.9
0.2
577
-2.8
0.3*
SC SEM 2.4 mg + LI
1306
1212
-15.3
NR
1232
-11.7
0.2
1212
-15.6
0.3*
STEP 1
(Extension)#
PBO→ Off Treatment
93
93
2
0.5
NR
NR
NR
93
2.1
0.5
SC SEM 2.4 mg + LI→
Off Treatment
197 197 12 0.6 NR NR NR 197 14.8 0.8
STEP 2
PBO + LI
403
376
-3.5
0.4
381
-2.7
0.2
376
-3.4
0.4
SC SEM 1.0 mg + LI
403
380
-6.9
0.4
378
-6.6
0.3
380
-7
0.4
SC SEM 2.4 mg + LI
404
388
-9.7
0.4
386
-8.7
0.3
388
-9.6
0.4
STEP 3
PBO + IBT
204
204
-6.2
NR
189
-7.9
0.5*
189
-5.8
0.4*
SC SEM 2.4 mg + IBT
407
407
-16.8
NR
380
-15.4
0.3*
373
-16.5
0.5*
STEP 4
Run-in period†
803
803
-11.1
0.2*
803
-10.6
0.2*
NR
NR
NR
From run-in with SEM→
PBO + LI‡
268 250 6.1 0.5* 265 -9.6 0.3* 268 6.9 0.5*
From run-in with SEM→ SC
SEM 2.4 mg + LI‡
535 520 -7.1 0.3* 531 -13.2 0.3* 535 -7.9 0.4*
STEP 5
PBO + LI
152
129
-3.5
0.7*
129
-2.6
NR
129
-3.3
0.6*
SC SEM 2.4 mg + LI
152
149
-16.7
0.8*
149
-12
NR
149
-15.8
0.8*
STEP 6
PBO + LI
101
100
-1.7
0.7
100
-2.4
0.4
101
-2.1
0.8
SC SEM 1.7 mg + LI
101
98
-8.2
0.7
99
-8.3
0.6
98
-9.6
0.8
SC SEM 2.4 mg + LI
199
193
-11.3
0.5
197
-10.1
0.4
193
-13.2
0.5
Semaglutide vs. Liraglutide
STEP 8
PBO + LI
85
78
-1.6
1.2*
NR
NR
NR
78
-1.9
1.1*
SC SEM 2.4 mg + LI
126
126
-15.3
1.0*
76
-13.3
NR
117
-15.8
0.9*
SC LIR 3.0 mg
127
127
-6.8
1.0*
66
-6.8
NR
117
-6.4
0.9*
Liraglutide
SCALE
(Maintenance)
PBO + LI
206
206
-0.1
0.5*
168
-1
0.5
144
-0.2
0.5*
SC LIR 3.0 mg + LI
207
207
-6
0.5*
181
-7.7
0.5
156
-6.2
0.5*
SCALE (Sleep
Apnea)§
PBO + LI
178
178
-1.9
0.4
178
-1.6
0.3
NR
NR
NR
SC LIR 3.0 mg + LI
175
175
-6.7
0.5
175
-5.7
0.4
NR
NR
NR
PBO + LI
211
116
-3.1
0.5*
137
-2.7
0.3*
211
-2
0.3*

©Institute for Clinical and Economic Review, 2022 Page D64
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
Change in Body Weight from
Baseline, Mean kg
Weight Loss from Baseline
to Six Months, Mean %
Weight Loss from Baseline
to One Year, Mean %
N
Mean
SE
N
Mean
SE
N
Mean
SE
SCALE (Type 2
Diabetes)
SC LIR 1.8 mg + LI
204
158
-5.2
0.5*
172
-4.9
0.3*
204
-4.6
0.4*
SC LIR 3.0 mg + LI
412
317
-7
0.3*
337
-6
0.3*
412
-5.9
0.3*
SCALE (Obesity
& Pre-
Diabetes)
PBO + LI
1225
1225
-2.8
6.5
1225
-2.9
0.3
1220
-2.6
0.2*
SC LIR 3.0 mg + LI 2437 2437 -8.4 7.3 2437 -8.2 0.2 2432 -8 0.1*
SCALE (IBT)
PBO + IBT
140
NR
NR
NR
128
-5.4
0.5
130
-4
0.6*
SC LIR 3.0 mg + IBT
142
NR
NR
NR
137
-8.4
0.6
141
-7.4
0.7*
SCALE (Insulin)
PBO + IBT
198
NR
NR
NR
183
-2.1
0.4
193
-1.5
0.4
SC LIR 3.0 mg + IBT
198
NR
NR
NR
188
-6.4
0.4
191
-5.8
0.4
LOSEIT
PBO + LI
76
76
1.2
1.2*
NR
NR
NR
NR
NR
NR
SC LIR 3.0 mg + LI
80
80
-2.8
1.3*
NR
NR
NR
NR
NR
NR
Phentermine/Topiramate
EQUIP
PBO + LI
498
NR
NR
NR
NR
NR
NR
498
-1.6
0.4
P/T 3.75 mg/23 mg + LI
234
NR
NR
NR
NR
NR
NR
234
-5.1
0.5
P/T 15 mg/92 mg + LI
498
NR
NR
NR
NR
NR
NR
498
-10.9
0.4
EQUATE
PBO + LI
103
103
-1.5
NR
103
-1.7
0.6
NR
NR
NR
Phentermine 7.5 mg + LI
104
104
-5.3
NR
104
-5.5
0.6
NR
NR
NR
Topiramate 46 mg + LI
102
102
-4.7
NR
102
-5.1
0.6
NR
NR
NR
P/T 7.5 mg/46 mg + LI
103
103
-8.3
NR
103
-8.5
0.6
NR
NR
NR
Phentermine 15 mg + LI
106
106
-6
NR
106
-6.1
0.6
NR
NR
NR
Topiramate 92 mg + LI
105
105
-6.4
NR
105
-6.4
0.6
NR
NR
NR
P/T 15 mg/92 mg + LI
103
103
-9
NR
103
-9.2
0.6
NR
NR
NR
CONQUER
(Diabetes
Subgroup)
PBO +LI
157
NR
NR
NR
NR
NR
NR
157
-1.9
0.6*
P/T 7.5 mg/46 mg + LI
67
NR
NR
NR
NR
NR
NR
67
-6.8
0.9*
P/T 15 mg/92 mg + LI
164
NR
NR
NR
NR
NR
NR
164
-8.8
0.6*
OB-204
(Winslow
2012)
PBO + LI
23
23
-4.7
1.2
23
-4.2
1.2
NR
NR
NR
P/T 15 mg/92 mg + LI 22 22 -11 1.2 22 -10.3 1.2 NR NR NR
Bupropion/Naltrexone
COR-I
PBO + LI
511
511
-1.4
0.3
NR
NR
NR
511
-1.3
0.3
B/N 360 mg/16 mg + LI
471
471
-4.9
0.3
NR
NR
NR
471
-5
0.3
B/N 360 mg/32 mg + LI
471
471
-6.1
0.3
NR
NR
NR
471
-6.1
0.3
COR-II
PBO + LI
456
456
-1.3
0.3
456
-1.9
0.3
456
-1.2
0.3

©Institute for Clinical and Economic Review, 2022 Page D65
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
Change in Body Weight from
Baseline, Mean kg
Weight Loss from Baseline
to Six Months, Mean %
Weight Loss from Baseline
to One Year, Mean %
N
Mean
SE
N
Mean
SE
N
Mean
SE
B/N 360 mg/32 mg + LI
702
702
-6.2
0.2
825
-6.5
0.2
702
-6.4
0.3
COR-BMOD
PBO + BMOD
202
NR
NR
NR
NR
-5.6
0.5
193
-5.1
0.6
B/N 360 mg/32 mg +
BMOD
591 NR NR NR NR -9.4 0.4 482 -9.3 0.4
COR-Diabetes
PBO + LI
159
NR
NR
NR
NR
-2
0.4
159
-1.8
0.4
B/N 360 mg/32 mg + LI
265
NR
NR
NR
NR
-5.1
0.3
265
-5
0.3
CVOT (Light
Study)
PBO + LI
4450
2848
-1.9
0.1*
3297
-1.7
NR
2848
-1.8
NR
B/N 360 mg/32 mg + LI
4455
2995
-4.9
0.1*
3404
-4.5
NR
2995
-4.6
NR
Ignite
Usual care (including LI)
82
82
-1
0.5
82
-0.9
0.5
NR
NR
NR
B/N 360 mg/32 mg + CLI
71
71
-9.5
0.6
71
-9.5
0.5
NR
NR
NR
BMOD: behavioral modification, B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, IBT: intensive behavioral therapy, KOA: knee
osteoarthritis, kg: kilogram, LI: lifestyle intervention, LIR: liraglutide, mg: milligram, N: total number, NR: not reported, PBO: placebo, P/T:
phentermine/topiramate, SC: subcutaneous, SE: standard error, SEM: semaglutide, vs.: versus
*SE manually derived from standard deviation or 95% CIs.
†Timepoint for outcomes is at Week 20.
‡Timepoint for outcomes is Week 20-68.
§Timepoint for all outcomes is at Week 32.
#Timepoint for all outcomes is Week 68-120.

©Institute for Clinical and Economic Review, 2022 Page D66
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D27. Efficacy: Weight Loss Outcomes II
29-38,40-45,48-52,54-57,59-67,72,140-144,147-149
Study Name Arms N
% Participants with 5% Body
Weight Loss
% Participants with 10% Body
Weight Loss
% Participants with 15% Body
Weight Loss
%
n
N
%
n
N
%
n
N
Semaglutide
STEP 1
PBO + LI
655
31.5
182
577
12
69
577
4.9
28
577
SC SEM 2.4 mg + LI
1306
86.4
1047
1212
69.1
838
1212
50.5
612
1212
STEP 1
(Extension)‡
PBO→ Off Treatment
93
22.6
21
93
NR
NR
NR
NR
NR
NR
SC SEM 2.4 mg + LI→
Off Treatment
197 48.2 95 197 NR NR NR NR NR NR
STEP 2
PBO + LI
403
28.5
107
376
8.2
31
376
3.2
12
376
SC SEM 1.0 mg + LI
403
57.1
217
380
28.7
109
380
13.7
52
380
SC SEM 2.4 mg + LI
404
68.8
267
388
45.6
177
388
25.8
100
388
STEP 3
PBO + IBT
204
47.6
90
189
27
51
189
13.2
25
189
SC SEM 2.4 mg + IBT
407
86.6
323
373
75.3
281
373
55.8
208
373
STEP 4
Run-in period
803
NR
NR
NR
NR
NR
NR
NR
NR
NR
From run-in with SEM→
PBO + LI*
268 47.6 119 250 20.4 51 250 9.2 23 250
From run-in with SEM→
SC SEM 2.4 mg + LI*
535 88.7 461 520 79 411 520 63.7 331 520
STEP 5
PBO + LI
152
29.5
38
129
13.2
17
129
5.4
7
129
SC SEM 2.4 mg + LI
152
88.6
132
149
68.5
102
149
52.3
78
149
STEP 6
PBO
101
21
21
100
5
5
100
3
3
100
SC SEM 1.7 mg + LI
101
72
71
98
42
41
98
24
24
98
SC SEM 2.4 mg + LI
199
83
160
193
61
117
193
41
79
193
Semaglutide vs. Liraglutide
STEP 8
PBO +LI
85
29.5
23
78
15.4
12
78
6.4
5
78
SC SEM 2.4 mg + LI
126
87.2
102
117
70.9
83
117
55.6
65
117
SC LIR 3.0 mg
127
58.1
68
117
25.6
30
117
12
14
117
Liraglutide
SCALE
(Maintenance)
PBO + LI
206
21.8
41
188
6.3
12
188
NR
NR
NR
SC LIR 3.0 mg + LI
207
50.5
98
194
26.1
51
194
NR
NR
NR
SCALE (Sleep
Apnea)†
PBO + LI
178
18.5
33
178
1.7
3
178
NR
NR
NR
SC LIR 3.0 mg + LI
175
46.3
81
175
23.4
41
175
NR
NR
NR
PBO + LI
211
21.4
45
211
6.7
14
211
NR
NR
NR

©Institute for Clinical and Economic Review, 2022 Page D67
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
% Participants with 5% Body
Weight Loss
% Participants with 10% Body
Weight Loss
% Participants with 15% Body
Weight Loss
%
n
N
%
n
N
%
n
N
SCALE (Type 2
Diabetes)
SC LIR 1.8 mg + LI
204
40.4
82
204
15.9
32
204
NR
NR
NR
SC LIR 3.0 mg + LI
412
54.3
224
412
25.2
104
412
NR
NR
NR
SCALE (Obesity
& Pre-
Diabetes)
PBO + LI
1225
27.1
331
1220
10.6
129
1220
NR
NR
NR
SC LIR 3.0 mg + LI 2437 63.2 1537 2432 33.1 805 2432 NR NR NR
SCALE (IBT)
PBO + IBT
140
38.8
50
130
19.8
26
130
8.9
12
130
SC LIR 3.0 mg + IBT
142
61.5
87
141
30.5
43
141
18.1
26
141
SCALE (Insulin)
PBO + IBT
198
24
46
193
6.6
13
193
NR
NR
NR
SC LIR 3.0 mg + IBT
198
51.8
100
191
22.8
44
191
NR
NR
NR
LOSEIT
PBO + LI
76
17.1
13
76
9.6
7
76
NR
NR
NR
SC LIR 3.0 mg + LI
80
35
28
80
21.3
17
80
NR
NR
NR
Phentermine/Topiramate
EQUIP
PBO +LI
498
17.3
86
498
7.4
37
498
3.4
17
498
P/T 3.75 mg/23 mg + LI
234
44.9
105
234
18.8
44
234
7.3
17
234
P/T 15 mg/92 mg + LI
498
66.7
332
498
47.2
235
498
32.3
161
498
EQUATE
PBO + LI
103
15.5
16
103
6.8
7
103
NR
NR
NR
Phentermine 7.5 mg + LI
104
43.3
45
104
12.5
13
104
NR
NR
NR
Topiramate 46 mg + LI
102
39.2
40
102
18.6
19
102
NR
NR
NR
P/T 7.5 mg/46 mg + LI
103
62.1
64
103
38.8
40
103
NR
NR
NR
Phentermine 15 mg + LI
106
46.2
49
106
20.8
22
106
NR
NR
NR
Topiramate 92 mg + LI
105
48.6
51
105
23.8
25
105
NR
NR
NR
P/T 15 mg/92 mg + LI
103
66
68
103
40.8
42
103
NR
NR
NR
CONQUER
(Diabetes
subgroup)
PBO + LI
157
NR
NR
NR
NR
NR
NR
NR
NR
NR
P/T 7.5 mg/46 mg + LI
67
NR
NR
NR
NR
NR
NR
NR
NR
NR
P/T 15 mg/92 mg + LI
164
NR
NR
NR
NR
NR
NR
NR
NR
NR
OB-204
(Winslow
2012)
PBO + LI
23
47.8
11
23
13
3
23
NR
NR
NR
P/T 15 mg/92 mg + LI 22 72.7 16 22 54.5 12 22 NR NR NR
Bupropion/Naltrexone
COR-I
PBO + LI
511
16
84
511
7
38
511
2
10
511
B/N 360 mg/16 mg + LI
471
39
186
471
20
95
471
9
41
471
B/N 360 mg/32 mg + LI
471
48
226
471
25
116
471
12
56
471
COR-II
PBO + LI
456
17.1
80
456
5.7
26
456
2.4
11
456

©Institute for Clinical and Economic Review, 2022 Page D68
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
% Participants with 5% Body
Weight Loss
% Participants with 10% Body
Weight Loss
% Participants with 15% Body
Weight Loss
%
n
N
%
n
N
%
n
N
B/N 360 mg/32 mg + LI
702
50.5
354
702
28.3
199
702
13.5
95
702
COR-BMOD
PBO + BMOD
202
42.5
82
193
20.2
39
193
10.9
21
193
B/N 360 mg/32 mg +
BMOD
591 66.4 320 482 41.5 200 482 29.1 140 482
COR-Diabetes
PBO + LI
159
18.9
30
159
5.7
9
159
NR
NR
NR
B/N 360 mg/32 mg + LI
265
44.5
118
265
18.5
49
265
NR
NR
NR
CVOT (Light
Study)
PBO + LI
4450
NR
NR
NR
NR
NR
NR
NR
NR
NR
B/N 360 mg/32 mg + LI
4455
NR
NR
NR
NR
NR
NR
NR
NR
NR
Ignite
Usual care (including LI)
82
12.2
10
82
3.7
3
82
0
0
82
B/N 360 mg/32 mg + CLI
71
84.5
60
71
42.3
30
71
12.7
9
71
BMOD: behavioral modification, B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, IBT: intensive behavioral therapy, KOA: knee
osteoarthritis, kg: kilogram, LI: lifestyle intervention, LIR: liraglutide, mg: milligram, n: number, N: total number, NR: not reported, PBO: placebo, P/T:
phentermine/topiramate, SC: subcutaneous, SEM: semaglutide, vs.: versus
*Timepoint for outcomes is Weeks 0-68.
†Timepoint for all outcomes is at Week 32.
‡Timepoint for all outcomes is Week 68-120.

©Institute for Clinical and Economic Review, 2022 Page D69
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D28. Efficacy: Secondary Outcomes I
29-38,40-45,48-67,72,140-149
Study Name Arms N
Change in A1C from Baseline, Mean %
Change in SBP from Baseline,
Mean mm Hg
Change in Waist
Circumference from
Baseline, cm
N
Mean
SE
N
Mean
SE
Mean
SE
Semaglutide
STEP 1
PBO + LI
655
563
-0.15
0.01*
577
-1.1
0.5*
-4.1
NR
SC SEM 2.4 mg + LI
1306
1197
-0.45
0.01*
1212
-6.2
0.4*
-13.5
NR
STEP 1
(Extension)¤
PBO→ Off Treatment
93
90
0.1
0.03
93
4
1.6
NR
NR
SC SEM 2.4 mg + LI→
Off Treatment
197 195 0.4 0.02 197 9 1.0 NR NR
STEP 2
PBO + LI
403
374
-0.4
0.1
376
-0.5
0.8
-4.5
0.4
SC SEM 1.0 mg + LI
403
376
-0.4
0.1
379
-2.9
0.9
-6.7
0.4
SC SEM 2.4 mg + LI
404
381
-0.4
0.1
387
-3.9
0.7
-9.4
0.4
STEP 3
PBO + IBT
204
204
-0.27
0.01*
188
-1.6
1.1*
-6.3
NR
SC SEM 2.4 mg + IBT
407
407
-0.51
0.02*
372
-5.6
0.7*
-14.6
NR
STEP 4
Run-in period†
803
803
-0.4
0.01*
803
-5.7
0.5*
-10.1
0.2*
From run-in with
SEM→ PBO + LI‡
268 246 0.1 0* 248 4.4 0.8* 3.3 0.5*
From run-in with
SEM→ SC SEM 2.4 mg
+ LI‡
535 515 -0.1 0.03* 518 0.5 0.6* -6.4 0.4*
STEP 5
PBO + LI
152
129
-0.2
0.02*
129
-1
1.2*
-4.5
0.6*
SC SEM 2.4 mg + LI
152
149
-0.5
0.03*
149
-7
1.1*
-14.3
0.8*
STEP 6
PBO + LI
101
100
-0.03
0.07
100
-5.3
1.2
-1.8
0.7
SC SEM 1.7 mg + LI
101
98
-0.89
0.07
98
-10.8
1.3
-7.7
0.7
SC SEM 2.4 mg + LI
199
193
-0.93
0.05
193
-10.8
0.9
-11.1
0.5
Semaglutide vs. Liraglutide
STEP 8
PBO + LI
85
76
0.1
0.02*
77
3.2
1.5*
-2
1.1*
SC SEM 2.4 mg + LI
126
113
-0.2
0.03*
114
-5.7
1.2*
-13.2
0.9*
SC LIR 3.0 mg
127
107
-0.1
0.03*
112
-2.9
1.2*
-6.6
0.9*
Liraglutide
SCALE
(Maintenance)
PBO + LI
206
206
0.1
0.03*
206
2.8
0.7*
-1.2
0.4*
SC LIR 3.0 mg + LI
207
207
-0.1
0.03*
207
0.2
0.8*
-4.7
0.5*
SCALE (Sleep
Apnea)§
PBO + LI
178
171
-0.2
0*
179
0
1
-3.1
0.5
SC LIR 3.0 mg + LI
175
174
-0.4
0
178
-3.4
0.9
-6.4
0.5
PBO + LI
211
211
-0.3
0.06*
211
-0.4
0.9*
-2.7
0.4*

©Institute for Clinical and Economic Review, 2022 Page D70
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
Change in A1C from Baseline, Mean %
Change in SBP from Baseline,
Mean mm Hg
Change in Waist
Circumference from
Baseline, cm
N
Mean
SE
N
Mean
SE
Mean
SE
SCALE (Type 2
Diabetes)
SC LIR 1.8 mg + LI
204
204
-1.1
0.07*
204
-3.5
0.9*
-4.8
0.4*
SC LIR 3.0 mg + LI
412
411
-1.3
0.04*
411
-2.8
0.7*
-6.1
0.3*
SCALE (Obesity
& Pre-Diabetes)
PBO + LI
1225
1225
-0.06
0.01*
1225
-1.5
0.4*
-3.9
0.2*
SC LIR 3.0 mg + LI
2437
2437
-0.3
0.01*
2437
-4.2
0.3*
-8.2
0.1*
SCALE (IBT)
PBO + IBT
140
140
-0.06
0.02*
130
-0.6
NR
-6.7
NR
SC LIR 3.0 mg + IBT
142
142
-0.16
0.03*
141
-2.8
NR
-9.4
NR
SCALE (Insulin)
PBO + IBT
198
188
-0.6
NR
198
-1.6
0.9
-2.6
NR
SC LIR 3.0 mg + IBT
198
187
-1.1
NR
198
-5.6
0.9
-5.3
NR
LOSEIT
PBO + LI
76
NR
NR
NR
NR
NR
NR
0.9
1.1*
SC LIR 3.0 mg + LI
80
NR
NR
NR
NR
NR
NR
-1.4
1.1*
Phentermine/Topiramate
EQUIP
PBO + LI
498
NR
NR
NR
498
0.9
0.6*
-3.1
0.5*
P/T 3.75 mg/23 mg + LI
234
NR
NR
NR
234
-1.8
0.8*
-5.6
0.6*
P/T 15 mg/92 mg + LI
498
NR
NR
NR
498
-2.9
0.6*
-10.9
0.5*
EQUATE
PBO + LI
103
87
0.1
0.02
103
-1.8
NR
-3.3
0.7
Phentermine 7.5 mg +
LI
104 89 0.1 0.02 104 -3.3 NR -6.4 0.7
Topiramate 46 mg + LI
102
89
0.1
0.02
102
-6.8
NR
-5.4
0.7
P/T 7.5 mg/46 mg + LI
103
91
0
0.02
102
-7
NR
-8.8#
0.7
Phentermine 15 mg +
LI
106 90 0.1 0.02 104 -3.5 NR -6.6 0.7
Topiramate 92 mg + LI
105
93
0
0.02
105
-6.4
NR
-6.2
0.7
P/T 15 mg/92 mg + LI
103
95
0
0.02
103
-5.2
NR
-8.7
0.7
CONQUER
(Diabetes
subgroup)
PBO +LI
157
144
-0.1
0.05
157
-2.1
1.1
NR
NR
P/T 7.5 mg/46 mg + LI
67
63
-0.4
1.5*
67
-2.9
1.6
NR
NR
P/T 15 mg/92 mg + LI
164
150
-0.4
0.6*
153
-4.2
1
NR
NR
OB-204
(Winslow 2012)
PBO + LI
23
NR
NR
NR
23
-7.3
2.6
NR
NR
P/T 15 mg/92 mg + LI 22 NR NR NR 22 -15 2.6 NR NR
Bupropion/Naltrexone
COR-I
PBO + LI
511
NR
NR
NR
511
-1.9
0.4
-2.5
0.4
B/N 360 mg/16 mg + LI
471
NR
NR
NR
471
0.3
0.4
-5
0.4
B/N 360 mg/32 mg + LI
471
NR
NR
NR
471
-0.1
0.4
-6.2
0.4

©Institute for Clinical and Economic Review, 2022 Page D71
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
Change in A1C from Baseline, Mean %
Change in SBP from Baseline,
Mean mm Hg
Change in Waist
Circumference from
Baseline, cm
N
Mean
SE
N
Mean
SE
Mean
SE
COR-II
PBO + LI
456
NR
NR
NR
456
-0.5
0.4
-2.1
0.5
B/N 360 mg/32 mg + LI
702
NR
NR
NR
702
0.6
0.3
-6.7
0.3
COR-BMOD
PBO + BMOD
202
NR
NR
NR
193
-3.9
0.7
-6.8
0.8*
B/N 360 mg/32 mg +
BMOD
591 NR NR NR 482 -1.3 0.5 -10 0.5*
COR-Diabetes
PBO + LI
159
137
-0.14
0.09
159
-1.1
0.9
-2.9
0.6
B/N 360 mg/32 mg + LI
265
222
-0.63
0.07
265
0
0.7
-5
0.5
CVOT (Light
Study)
PBO + LI
4450
NR
NR
NR
2850
1
0.3*
-0.8
0.1*
B/N 360 mg/32 mg + LI
4455
NR
NR
NR
2997
1.2
0.3*
-2.1
0.2*
Ignite
Usual care (including
LI)
82 NR NR NR 82 -2.8 1 -1.6 0.7
B/N 360 mg/32 mg +
CLI
71 NR NR NR 71 -4.8 1.1 -7 0.7
A1C: glycated hemoglobin, BMOD: behavioral modification, B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, cm: centimeter, IBT: intensive
behavioral therapy, KOA: knee osteoarthritis, kg: kilogram, LI: lifestyle intervention, LIR: liraglutide, mg: milligram, N: total number, NR: not reported, PBO: placebo,
P/T: phentermine/topiramate, SBP: systolic blood pressure, SC: subcutaneous, SE: standard error, SEM: semaglutide, vs.: versus
*SE manually derived from standard deviation or 95% CIs.
†Timepoint for outcomes is at Week 20.
‡Timepoint for outcomes is Week 20-68.
§Timepoint for all outcomes is at Week 32.
#The number of patients for this outcome may differ from the primary analysis population.
¤Timepoint for all outcomes is Week 68-120.

©Institute for Clinical and Economic Review, 2022 Page D72
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D29. Efficacy: Secondary Outcomes II
29-38,40-45,48-67,72,140-149
Study Name Arms N
Change in LDL from Baseline,
mg/dL
Ratio of LDL from Baseline
Change in Blood
Glucose, mg/dL
Change in BMI, kg/m2
N
Mean
SE
N
Mean
SE
Mean
SE
Mean
SE
Semaglutide
STEP 1
PBO + LI
655
561
1.1
NR
561
1.01
NR
-0.5
NR
-0.9
NR
SC SEM 2.4 mg + LI
1306
1194
-3.3
NR
1194
0.97
NR
-8.4
NR
-5.5
NR
STEP 1
(Extension)††
PBO→ Off Treatment
93
NR
NR
NR
92
0.95
NR
NR
NR
0.7
0.2
SC SEM 2.4 mg + LI→
Off Treatment
197 NR NR NR 194 1.01 NR NR NR 4.3 0.2
STEP 2
PBO + LI
403
374
0
NR
374
1.00
NR
-0.1
1.8
-1.3
0.1
SC SEM 1.0 mg + LI
403
376
-0.9
NR
376
0.99
NR
-1.8
1.8
-2.5
0.1
SC SEM 2.4 mg + LI
404
382
0
NR
382
1.00
NR
-2.1
1.8
-3.5
0.1
STEP 3
PBO + IBT
204
204
2.6
NR
NR
NR
NR
-0.7
NR
-2.2
NR
SC SEM 2.4 mg + IBT
407
407
-4.7
NR
NR
NR
NR
-6.7
NR
-6.0
NR
STEP 4
Run-in period† 803 NR NR NR 798 1
IQR:
0.8-1.1
-9.5 0.4* -4.0 0.1*
From run-in with
SEM→ PBO + LI‡
268 245 8 1.3* NR NR NR 6.7 0.9* 2.2 0.2*
From run-in with
SEM→ SC SEM 2.4 mg
+ LI‡
535 517 1 1.0* NR NR NR -0.8 0.5* -2.6 0.1*
STEP 5
PBO + LI
152
129
-1.1
NR
129
0.99
NR
1.6*
NR
-1.3
0.2*
SC SEM 2.4 mg + LI
152
149
-7.8
NR
149
0.93
NR
-7.6*
NR
-6
0.3*
STEP 6
PBO
101
NR
NR
NR
99
0.96
NR
2.2
1.6
-0.6
0.2
SC SEM 1.7 mg+ LI
101
NR
NR
NR
98
0.90
NR
-17.8
1.8
-3.1
0.2
SC SEM 2.4 mg+ LI
199
NR
NR
NR
193
0.85
NR
-19.6
1.3
-4.2
0.2
Semaglutide vs. Liraglutide
STEP 8
PBO +LI
85
74
-1.1
5.6*
NR
NR
NR
3.3
1.4*
NR
NR
SC SEM 2.4 mg + LI
126
112
-6.5
3.1*
NR
NR
NR
-8.3
1.1*
NR
NR
SC LIR 3.0 mg
127
107
0.9
2.8*
NR
NR
NR
-4.3
1.2*
NR
NR
Liraglutide
SCALE
(Maintenance)
PBO + LI
206
206
11.6
1.6*
NR
NR
NR
-3.6
0.9*
0
0.2*
SC LIR 3.0 mg + LI
207
207
7.7
1.6*
NR
NR
NR
-9.0
0.8*
-2.1
0.2*
SCALE (Sleep
Apnea)§
PBO + LI
178
NR
NR
NR
NR
NR
NR
3.6
1.8
-0.6
0.1
SC LIR 3.0 mg + LI
175
NR
NR
NR
NR
NR
NR
-3.6
1.8
-2.2
0.2
SCALE (Type 2
Diabetes)
PBO + LI
211
211
5
NR
NR
NR
NR
-0.2
2.6*
-0.8
0.1*
SC LIR 1.8 mg + LI
204
204
-3.1
NR
NR
NR
NR
-26.8
3.5*
-1.7
0.1*
SC LIR 3.0 mg + LI
412
411
0.6
NR
NR
NR
NR
-34.3
1.9*
-2.2
0.1*

©Institute for Clinical and Economic Review, 2022 Page D73
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
Change in LDL from Baseline,
mg/dL
Ratio of LDL from Baseline
Change in Blood
Glucose, mg/dL
Change in BMI, kg/m2
N
Mean
SE
N
Mean
SE
Mean
SE
Mean
SE
SCALE (Obesity
& Pre-Diabetes)
PBO + LI
1225
1225
-1
NR
NR
NR
NR
0.1
0.3*
-1.0
0.1*
SC LIR 3.0 mg + LI
2437
2437
-3
NR
NR
NR
NR
-7.1
0.2*
-3.0
0.1*
SCALE (IBT)
PBO + IBT
140
130
1.5
NR
NR
NR
NR
0.2
NR
NR
NR
SC LIR 3.0 mg + IBT
142
141
-1.5
NR
NR
NR
NR
-4.1
NR
NR
NR
SCALE (Insulin)
PBO + IBT
198
190
0.9
NR
190
1.01
NR
-11.5
NR
NR
NR
SC LIR 3.0 mg + IBT
198
186
-2.8
NR
186
0.97
NR
-18.4
NR
NR
NR
LOSEIT
PBO + LI
76
NR
NR
NR
NR
NR
NR
NR
NR
0.3
0.4*
SC LIR 3.0 mg + LI
80
NR
NR
NR
NR
NR
NR
NR
NR
-1.0
0.4*
Phentermine/Topiramate
EQUIP
PBO +LI
498
478
-5.5¤
0.9*
NR
NR
NR
1.9
0.5*
NR
NR
P/T 3.75 mg/23 mg +
LI
234 230 -7.7¤ 1.3* NR NR NR 0.8 0.7* NR NR
P/T 15 mg/92 mg + LI
498
486
-8.4¤
0.9*
NR
NR
NR
-0.6
0.5*
NR
NR
EQUATE
PBO + LI
103
NR
NR
NR
NR
NR
NR
-0.1**
0.1
NR
NR
Phentermine 7.5 mg +
LI
104 NR NR NR NR NR NR 0.0** 0.1 NR NR
Topiramate 46 mg + LI
102
NR
NR
NR
NR
NR
NR
0.0**
0.1
NR
NR
P/T 7.5 mg/46 mg + LI
103
NR
NR
NR
NR
NR
NR
0.0**
0.1
NR
NR
Phentermine 15 mg +
LI
106 NR NR NR NR NR NR -0.1** 0.1 NR NR
Topiramate 92 mg + LI
105
NR
NR
NR
NR
NR
NR
0.0**
0.1
NR
NR
P/T 15 mg/92 mg + LI
103
NR
NR
NR
NR
NR
NR
-0.1**
0.1
NR
NR
CONQUER
(Diabetes
Subgroup)
PBO + LI
157
152
-2.3
2.1
NR
NR
NR
-5.4
1.8*
NR
NR
P/T 7.5 mg/46 mg + LI
67
65
-3.6
3.2
NR
NR
NR
-9
3.6*
NR
NR
P/T 15 mg/92 mg + LI
164
158
-2.8
2
NR
NR
NR
-12.6
1.8*
NR
NR
OB-204
(Winslow 2012)
PBO + LI
23
22
-1.6
5.6
NR
NR
NR
-5.6
5.9
NR
NR
P/T 15 mg/92 mg + LI
22
21
-11
6
NR
NR
NR
-8.9
6.1
NR
NR
Bupropion/Naltrexone
COR-I
PBO + LI
511
345
-3.3
1.2
NR
NR
NR
-1.3
0.6
NR
NR
B/N 360 mg/16 mg +
LI
471 332 -3.7 1.2 NR NR NR -2.4 0.6 NR NR
B/N 360 mg/32 mg +
LI
471 358 -4.4 1.2 NR NR NR -3.2 0.6 NR NR
COR-II
PBO + LI
456
456
-2.1
1.3
NR
NR
NR
-1.3
0.6
NR
NR
B/N 360 mg/32 mg +
LI
702 702 -6.2 0.9 NR NR NR -2.8 0.5 NR NR
COR-BMOD
PBO + BMOD
202
143
8.1
2.1
NR
NR
NR
-1.1
1.0
NR
NR

©Institute for Clinical and Economic Review, 2022 Page D74
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
Change in LDL from Baseline,
mg/dL
Ratio of LDL from Baseline
Change in Blood
Glucose, mg/dL
Change in BMI, kg/m2
N
Mean
SE
N
Mean
SE
Mean
SE
Mean
SE
B/N 360 mg/32 mg +
BMOD
591 392 5.4 1.4 NR NR NR -2.4 0.6 NR NR
COR-Diabetes
PBO + LI
159
134
0
2.4
NR
NR
NR
-4
3.4
NR
NR
B/N 360 mg/32 mg +
LI
265 220 -1.4 1.9 NR NR NR -11.9 2.7 NR NR
CVOT (Light
Study)
PBO + LI
4450
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
B/N 360 mg/32 mg +
LI
4455 NR NR NR NR NR NR NR NR NR NR
Ignite
Usual care (including
LI)
82 82 -1.9 2.1 NR NR NR 1.6 1.0 NR NR
B/N 360 mg/32 mg +
CLI
71 71 -2 2.2 NR NR NR -2.9 1.0 NR NR
BMI: body-mass index, BMOD: behavioral modification, B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, IBT: intensive behavioral therapy, IQR:
interquartile range, kg: kilogram, KOA: knee osteoarthritis, kg: kilogram, LDL: low-density lipoprotein, LI: lifestyle intervention, LIR: liraglutide, m: meter, mg: milligram, N: total
number, NR: not reported, PBO: placebo, P/T: phentermine/topiramate, SC: subcutaneous, SE: standard error, SEM: semaglutide, vs.: versus
*SE manually derived from standard deviation or 95% CIs.
†Timepoint for outcomes is at Week 20.
‡Timepoint for outcomes is Week 20-68.
§Timepoint for all outcomes is at Week 32.
#Timepoint for this outcome is at Week 104.
¤Percent change.
**The number of patients for this outcome may differ from the primary analysis population.
††Timepoint for all outcomes is Week 68-120.

©Institute for Clinical and Economic Review, 2022 Page D75
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D30. Patient-Reported Outcomes
29-32,34,35,41-45,48,50-52,54-57,59-67,140-142,144,147-149
Study Name Arms N
SF-36, Change from Baseline
IWQOL-Lite-CT, Change from
Baseline
Depression
Score, Change
from Baseline
Physical
Functioning
Score
Physical
Component
Score
Mental
Component
Score
Physical
Function
Score
Total Score
Mean
SE
Mean
SE
Mean
SE
Mean
SE
Mean
SE
Mean
SE
Semaglutide
STEP 1
PBO + LI
655
0.4
NR
0.2*
0.3†
-2.1*
0.3†
5.3
NR
NR
NR
NR
NR
SC SEM 2.4 mg + LI
1306
2.2
NR
2.4*
0.2†
-1.5*
0.2†
14.7
NR
NR
NR
NR
NR
STEP 2
PBO + LI
403
1*
0.4
NR
NR
NR
NR
5.3
1.1
NR
NR
NR
NR
SC SEM 2.4 mg + LI
404
2.5*
0.4
NR
NR
NR
NR
10.1
1
NR
NR
NR
NR
STEP 3
PBO + IBT
204
1.6
NR
2.3
NR
-2.9
NR
NR
NR
NR
NR
NR
NR
SC SEM 2.4 mg + IBT
407
2.4
NR
3
NR
-0.8
NR
NR
NR
NR
NR
NR
NR
STEP 4
Run-in period#
803
2.2
5.1†
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
From run-in with SEM→
PBO + LI¤
268 -1.5 0.4† -0.9 0.5† -3.4 0.5† NR NR NR NR NR NR
From run-in with SEM→
SC SEM 2.4 mg + LI¤
535 1 0.2† 0.8 0.3† 0.1 0.3† NR NR NR NR NR NR
STEP 5
PBO + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
SC SEM 2.4 mg + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
STEP 6
PBO + LI
101
-0.3
0.4
NR
NR
NR
NR
0.8
1.4
NR
NR
NR
NR
SC SEM 1.7 mg + LI
101
-0.1
0.5
NR
NR
NR
NR
2.8
1.5
NR
NR
NR
NR
SC SEM 2.4 mg + LI
199
0.8
0.3
NR
NR
NR
NR
4.2
1.1
NR
NR
NR
NR
Semaglutide vs. Liraglutide
STEP 8
PBO + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
SC SEM 2.4 mg + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
SC LIR 3.0 mg
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Liraglutide
SCALE
(Maintenance)
PBO + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
SC LIR 3.0 mg + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
SCALE (Sleep
Apnea)**
PBO + LI
171
NR
NR
1.9
0.5
0.9
0.6
NR
NR
NR
NR
NR
NR
SC LIR 3.0 mg + LI
174
NR
NR
3
0.6
1.4
0.6
NR
NR
NR
NR
NR
NR
SCALE (Type 2
Diabetes)
PBO + LI
211
NR
NR
NR
NR
NR
NR
8.9
1.1†
7.6
0.9†
NR
NR
SC LIR 1.8 mg + LI
204
NR
NR
NR
NR
NR
NR
12.5
1.2†
9.1
1.0†
NR
NR

©Institute for Clinical and Economic Review, 2022 Page D76
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
SF-36, Change from Baseline
IWQOL-Lite-CT, Change from
Baseline
Depression
Score, Change
from Baseline
Physical
Functioning
Score
Physical
Component
Score
Mental
Component
Score
Physical
Function
Score
Total Score
Mean
SE
Mean
SE
Mean
SE
Mean
SE
Mean
SE
Mean
SE
SC LIR 3.0 mg + LI
411
NR
NR
NR
NR
NR
NR
15.2
0.9†
11.7
0.7†
NR
NR
SCALE (Obesity
& Pre-Diabetes)
PBO + LI
1225
NR
NR
2.1
0.2†
-0.9
0.3†
NR
NR
7.7
0.4†
NR
NR
SC LIR 3.0 mg + LI
2437
NR
NR
3.6
0.1†
0.2
0.2†
NR
NR
10.6
0.3†
NR
NR
SCALE (IBT)
PBO + IBT
140
3.8
NR
3.8
0.6†
-2.2
0.7†
14.1†
NR
12.8
1.7†
NR
NR
SC LIR 3.0 mg + IBT
142
4
NR
3.4
0.6†
-1.2
0.7†
14.9†
NR
13.2
1.6†
NR
NR
SCALE (Insulin)
PBO + IBT
198
2.6
0.5†
2.2
0.5†
-1.7
0.5†
5.7†
NR
4.8
1.2†
NR
NR
SC LIR 3.0 mg + IBT
198
2.5
0.6†
2.7
0.5†
-1.9
0.6†
8.2†
NR
5.7
1.3†
NR
NR
LOSEIT
PBO + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
SC LIR 3.0 mg + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Phentermine/Topiramate
EQUIP
PBO + LI
498
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.3*‡
0.2†
P/T 3.75 mg/23 mg + LI
234
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.2*‡
0.2†
P/T 15 mg/92 mg + LI
498
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.5*‡
0.1†
EQUATE
PBO + LI
101
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-0.5*‡
0.4†
Phentermine 7.5 mg + LI
103
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.1*‡
0.3†
Topiramate 46 mg + LI
102
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.1*‡
0.3†
P/T 7.5 mg/46 mg + LI
95
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.3*‡
0.2†
Phentermine 15 mg + LI
104
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.4*‡
0.4†
Topiramate 92 mg + LI
103
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.7*‡
0.3†
P/T 15 mg/92 mg + LI
103
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
-1.1*‡
0.4†
CONQUER
(Diabetes
Subgroup)
PBO + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
P/T 7.5 mg/46 mg + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
P/T 15 mg/92 mg + LI
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
OB-204
(Winslow 2012)
PBO + LI
22
4.5
2.9
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
P/T 15 mg/92 mg + LI
21
9.2
2.9
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Bupropion/Naltrexone
COR-I
PBO + LI
511
NR
NR
NR
NR
NR
NR
NR
NR
8.6*
0.5
-0.7*§
0.2
B/N 360 mg/16 mg + LI
471
NR
NR
NR
NR
NR
NR
NR
NR
11.7*
0.5
0*§
0.2
B/N 360 mg/32 mg + LI
471
NR
NR
NR
NR
NR
NR
NR
NR
12.7*
0.5
-0.3*§
0.2
COR-II
PBO + LI
456
NR
NR
NR
NR
NR
NR
8.2
0.8
6.4
0.6
-0.5*§
0.3

©Institute for Clinical and Economic Review, 2022 Page D77
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
SF-36, Change from Baseline
IWQOL-Lite-CT, Change from
Baseline
Depression
Score, Change
from Baseline
Physical
Functioning
Score
Physical
Component
Score
Mental
Component
Score
Physical
Function
Score
Total Score
Mean
SE
Mean
SE
Mean
SE
Mean
SE
Mean
SE
Mean
SE
B/N 360 mg/32 mg + LI
702
NR
NR
NR
NR
NR
NR
14.1
0.6
10.9
0.5
-0.3*§
0.2
COR-BMOD
PBO + BMOD
202
NR
NR
NR
NR
NR
NR
12
0.8
10.3*
0.9
0*§
0.4
B/N 360 mg/32 mg +
BMOD
591 NR NR NR NR NR NR 16.5 0.5 13.4* 0.6 0.1*§ 0.2
COR-Diabetes
PBO + LI
159
NR
NR
NR
NR
NR
NR
NR
NR
7.9*
0.9
-1.6*§
0.4
B/N 360 mg/32 mg + LI
265
NR
NR
NR
NR
NR
NR
NR
NR
9.3*
0.7
0*§
0.3
CVOT (Light
Study)
PBO + LI
4450
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
B/N 360 mg/32 mg + LI
4455
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Ignite
Usual care (including LI)
82
NR
NR
NR
NR
NR
NR
NR
NR
-1
1.4
NR
NR
B/N 360 mg/32 mg + CLI
71
NR
NR
NR
NR
NR
NR
NR
NR
16.4
1.5
NR
NR
BMOD: behavioral modification, B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, IBT: intensive behavioral therapy, IWQOL-Lite: Impact
of Weight on Quality of Life-Lite, KOA: knee osteoarthritis, kg: kilogram, LI: lifestyle intervention, LIR: liraglutide, mg: milligram, N: total number, NR: not
reported, PBO: placebo, P/T: phentermine/topiramate, SC: subcutaneous, SE: standard error, SEM: semaglutide, SF-36: Short Form Health Survey, vs.: versus
*The number of patients for this outcome may differ from the primary analysis population.
†SE manually derived from standard deviation or 95% CIs.
‡Depression for this trial is measured by the PHQ-9.
§Depression for this trial is measured by the IDS-SR.
#Timepoint for outcomes is at week 20.
¤Timepoint for outcomes is week 20-68.
**Timepoint for all outcomes is at week 32.
©Institute for Clinical and Economic Review, 2022 Page D78
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D31. Patient-Reported Outcomes of Sleep Apnea Studies
41,50,144,148
Study Name Arms N
ESS
FOSQ
PSQI
Mean
SE
Mean
SE
Mean
SE
Liraglutide
SCALE (Sleep Apnea)
PBO + LI
171
-2.3
0.3
1.1
0.1
NR
NR
SC LIR 3.0 mg + LI
174
-2.5
0.3
1.3
0.2
NR
NR
Phentermine/Topiramate
OB-204 (Winslow 2012)
PBO + LI
22
-1.8
0.8
NR
NR
-0.9
0.7
P/T 15 mg/92 mg + LI
21
-1.9
0.8
NR
NR
-3.1
0.7
ESS: Epworth Sleepiness Scale, FOSQ: Functional Outcomes of Sleep Questionnaire, LI: lifestyle intervention, LIR: liraglutide, mg: milligram, N: total number,
NR: not reported, PBO: placebo, PSQI: Pittsburgh Sleep Quality Index, P/T: phentermine/topiramate, SC: subcutaneous, SE: standard error

©Institute for Clinical and Economic Review, 2022 Page D79
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D32. Safety
29-38,40-45,48-66,140-149
Study Name Arms N
Any Adverse Events Serious Adverse Events
Adverse Events Leading to
Discontinuation
n
%
n
%
n
%
Semaglutide
STEP 1
PBO + LI
655
566
86.4
42
6.4
20
3.1
SC SEM 2.4 mg + LI
1306
1171
89.7
128
9.8
92
7
STEP 2
PBO + LI
402
309
76.9
37
9.2
14
3.5
SC SEM 2.4 mg + LI
403
353
87.6
40
9.9
25
6.2
STEP 3
PBO + IBT
204
196
96.1
6
2.9
6
2.9
SC SEM 2.4 mg + IBT
407
390
95.8
37
9.1
24
5.9
STEP 4
Run-in period†
902
760
84.3
21
2.3
48
5.3
From run-in with SEM→
PBO + LI‡
268 201 75 15 5.6 6 2.2
From run-in with SEM→
SC SEM 2.4 mg + LI‡
535 435 81.3 41 7.7 13 2.4
STEP 5
PBO + LI
152
136
89.5
18
11.8
7
4.6
SC SEM 2.4 mg + LI
152
146
96.1
12
7.9
9
5.9
STEP 6
PBO + LI
101
80
79
7
7
1
1
SC SEM 1.7 mg + LI
100
82
82
7
7
3
3
SC SEM 2.4 mg + LI
199
171
86
10
5
5
3
Semaglutide vs. Liraglutide
STEP 8
PBO + LI
85
81
95.3
6
7.1
3
3.5
SC SEM 2.4 mg + LI
126
120
95.2
10
7.9
4
3.2
SC LIR 3.0 mg
127
122
96.1
14
11
16
12.6
Liraglutide
SCALE
(Maintenance)
PBO + LI
210
186
88.6
5
2.4
18
8.6
SC LIR 3.0 mg + LI
212
194
91.5
9
4.3
18
8.5
SCALE (Sleep
Apnea)
PBO + LI
179
124
69.3
6
3.4
NR
NR
SC LIR 3.0 mg + LI
176
141
80.1
6
3.4
NR
NR
SCALE (Type 2
Diabetes)
PBO + LI
212
182
85.8
21
9.9
7
3.3
SC LIR 1.8 mg + LI
210
190
90.5
29
13.8
18
8.6
SC LIR 3.0 mg + LI
422
392
92.9
52
12.3
39
9.2
SCALE (Obesity &
Pre-Diabetes)
PBO + LI
1242
786
63.3
62
5
47
3.8
SC LIR 3.0 mg + LI
2481
1992
80.3
154
6.2
240*
9.7

©Institute for Clinical and Economic Review, 2022 Page D80
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
Any Adverse Events Serious Adverse Events
Adverse Events Leading to
Discontinuation
n
%
n
%
n
%
SCALE (IBT)
PBO + IBT
140
124
88.6
2
1.4
6
4.3
SC LIR 3.0 mg + IBT
142
136
95.8
6
4.2
12
8.5
SCALE (Insulin)
PBO + IBT
197
175
88.8
19
9.6
6
3
SC LIR 3.0 mg + IBT
195
180
92.3
16
8.2
15
7.7
LOSEIT
PBO + LI
76
71
93
6
8
4
5.3
SC LIR 3.0 mg + LI
80
77
96
7
9
10
12.5
Phentermine/Topiramate
EQUIP
PBO + LI
513
374
72.9
13
2.5
43
8.4
P/T 3.75 mg/23 mg + LI
240
192
80
6
2.5
27
11.3
P/T 15 mg/92 mg + LI
511
432
84.5
13
2.5
82
16
EQUATE
PBO + LI
109
87
79.8
0
0
8
7.3
Phentermine 7.5 mg + LI
109
87
79.8
2
1.8
10
9.2
Topiramate 46 mg + LI
106
90
84.9
0
0
8
7.4
P/T 7.5 mg/46 mg + LI
106
85
80.2
1
0.9
16
15.1
Phentermine 15 mg + LI
108
89
82.4
1
0.9
11
10.2
Topiramate 92 mg + LI
107
85
79.4
1
0.9
18
16.8
P/T 15 mg/92 mg + LI
108
90
83.3
2
1.9
23
21.3
CONQUER
(Diabetes
subgroup)
PBO + LI
157
125
79.6
5
3.2
13
8.3
P/T 7.5 mg/46 mg + LI
67
54
80.6
4
6
6
9
P/T 15 mg/92 mg + LI
164
141
86
6
3.7
31
18.9
OB-204 (Winslow
2012)
PBO + LI
23
18
78.2
1
4.4
1
4.3
P/T 15 mg/92 mg + LI
22
20
90.9
0
0
2
9.1
Bupropion/Naltrexone
COR-I
PBO + LI
569
390
68.5
8
1.4
56
9.8
B/N 360 mg/16 mg + LI
569
455
80
9
1.6
122
21.4
B/N 360 mg/32 mg + LI
573
476
83.1
9
1.6
112
19.5
COR-II
PBO + LI
492
370
75.2
7
1.4
68
13.8
B/N 360 mg/32 mg + LI
992
852
85.9
21
2.1
241
24.3
COR-BMOD
PBO + BMOD
200
133
66.5
1
0.5
25*
12.4
B/N 360 mg/32 mg + BMOD
584
487
83.4
22
3.8
150*
25.4
COR-Diabetes
PBO + LI
169
144
85.2
13
4.7
26
15.4
B/N 360 mg/32 mg + LI
333
301
90.4
8
3.9
98
29.4
PBO + LI
4450
668
15
386
8.7
388
8.7

©Institute for Clinical and Economic Review, 2022 Page D81
Evidence Report – Medications for Obesity Management Return to Table of Contents
Study Name Arms N
Any Adverse Events Serious Adverse Events
Adverse Events Leading to
Discontinuation
n
%
n
%
n
%
CVOT (Light
Study)
B/N 360 mg/32 mg + LI 4455 1620 36.4 463 10.4 1253 28.1
Ignite
Usual care (including LI)§
89
NR
NR
0
0
1
1.1
B/N 360 mg/32 mg + CLI§
153
NR
NR
1
0.7
35
22.9
Usual care (including LI)→B/N
360 mg/32 mg + CLI‡
89 NR NR 0 0 14 15.7
B/N 360 mg/32 mg + CLI
(continued)‡
153 NR NR 2 1.3 37 24.2
BMOD: behavioral modification, B/N: bupropion/naltrexone, CLI: comprehensive lifestyle intervention, IBT: intensive behavioral therapy, KOA: knee osteoarthritis, LI: lifestyle
intervention, LIR: liraglutide, mg: milligram,
n: number, N: total number, NR: not reported, PBO: placebo, P/T: phentermine/topiramate, SC: subcutaneous, SEM: semaglutide,
vs.: versus
*The number of patients for this outcome may differ from the safety analysis population.
†Timepoint for outcomes is at week 20.
‡Timepoint for outcomes is week 20-68.
§Timepoint for all outcomes is at week 26.
‡Timepoint for all outcomes is at week 78.

©Institute for Clinical and Economic Review, 2022 Page D82
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table D33. Safety Focus Areas for STEP Trials of Semaglutide
29-31,33-38,68
STEP 1
STEP 2*
STEP 3
STEP 5
STEP 8
Study Arms
PBO
SEM
PBO
SEM
PBO
SEM
PBO
SEM
PBO
SEM
LIR
N
655
1306
402
403
204
407
152
152
85
126
127
GI Disorders,
n (%)
314
(47.9)
969
(74.2)
138
(34.3)
256
(63.5)
129
(63.2)
337
(82.8)
82 (53.9)
125
(82.2)
47 (55.3)
106
(84.1)
105
(82.7)
Gallbladder-
Related
Disorders, n (%)
8 (1.2) 34 (2.6) 3 (0.7) 1 (0.2) 3 (1.5) 20 (4.9) 2 (1.3) 4 (2.6) 1 (1.2) 1 (0.8) 4 (3.1)
Hepatic
Disorders, n (%)
20 (3.1) 31 (2.4) 14 (3.5) 10 (2.5) 4 (2) 8 (2) 3 (2) 3 (2) 3 (3.5) 2 (1.6) 1 (0.8)
Acute
Pancreatitis,
n (%)
0 (0) 3 (0.2) 1 (0.2) 1 (0.2) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 1 (0.8)
CV Disorders,
n (%)
75 (11.5) 107 (8.2) 5 (1.2) 6 (1.5) 22 (10.8) 40 (9.8) 30 (19.7) 17 (11.2) 9 (10.6) 16 (12.7) 18 (14.2)
Psychiatric
Disorders, n (%)
83 (12.7) 124 (9.5) 15 (3.7) 24 (6) 24 (11.8) 60 (14.7) 25 (16.4) 26 (17.1) 9 (10.6) 7 (5.6) 19 (15)
Acute Renal
Failure, n (%)
2 (0.3) 3 (0.2) 2 (0.5) 4 (1) 0 (0) 0 (0) 0 (0) 0 (0) 1 (1.2) 1 (0.8) 0 (0)
Retinal
Disorders, n (%)
NR (NR) NR (NR) 17 (4.2) 28 (6.9) NR (NR) NR (NR) NR (NR) NR (NR) NR (NR) NR (NR) NR (NR)
CV: cardiovascular, GI: gastrointestinal, LIR: liraglutide, n: number, N: total number, NR: not reported, PBO: placebo
*Trial conducted in individuals with obesity and type 2 diabetes mellitus.

©Institute for Clinical and Economic Review, 2022 Page D83
Evidence Report – Medications for Obesity Management Return to Table of Contents
D4. Ongoing Studies
Table D34. Ongoing Studies
Title/Trial Sponsor Study Design Treatment Arms Patient Population Primary Outcome(s)
Estimated
Completion
Date
Semaglutide
Semaglutide Effects
on Heart Disease and
Stroke in Patients
With Overweight or
Obesity (SELECT)
Novo Nordisk
NCT03574597
Phase III
MC, QB, PC,
RCT
N~17,500
Semaglutide 2.4 mg
Placebo
Inclusion Criteria
• Male or female, age ≥45 years
• BMI ≥27 kg/m
2
• Have established CV disease with ≥1 of following:
prior MI; prior stroke; or symptomatic PAD, or
peripheral arterial revascularization procedure, or
amputation due to atherosclerotic disease
Exclusion Criteria
• MI, stroke, hospitalization for unstable angina
pectoris or transient ischemic attack within past 60
days
• HbA1C≥ 48 mmol/mol (6.5%)
• History of T1DM or T2DM (history of gestational
diabetes is allowed)
• Time to first
occurrence of a
composite
endpoint
consisting of: CV
death, non-fatal
MI, or non-fatal
stroke [0-59
months]
September
2023
Research Study to
Investigate How Well
Semaglutide Works in
People Living With
Heart Failure and
Obesity (STEP-HFpEF)
Novo Nordisk
NCT04788511
Phase III
MC, DB, PC,
RCT
N~516
Semaglutide 2.4 mg
Placebo
Inclusion Criteria
• Male or female, age ≥18 years
• BMI ≥30.0 kg/m
2
• NYHA Class II-IV
• LVEF ≥45%
Exclusion Criteria
• Change in body weight >5 kg (11 lbs) within 90 days
• HbA1C ≥6.5% (48 mmol/mol)
• Change in KCCQ
clinical summary
score [week 0-
52]
• Change in body
weight [week 0-
52]
March 2023
Research Study to
Look at How Well
Semaglutide Works in
People Living With
Heart Failure, Obesity
and Type 2 Diabetes
(STEP HFpEF DM)
Phase III
MC, QB, PC,
RCT
N~610
Semaglutide 2.4 mg
Placebo
Inclusion Criteria
• Male or female, age ≥18 years
• BMI ≥30.0 kg/m
2
• NYHA Class II-IV
• LVEF ≥45%
• Diagnosed with T2DM
• HbA1C ≤10%
• Change in KCCQ
clinical summary
score [week 0-
52]
• Change in body
weight [week 0-
52]
June 2023

©Institute for Clinical and Economic Review, 2022 Page D84
Evidence Report – Medications for Obesity Management Return to Table of Contents
Title/Trial Sponsor Study Design Treatment Arms Patient Population Primary Outcome(s)
Estimated
Completion
Date
Novo Nordisk
NCT04916470
Exclusion Criteria
• Change in body weight >5 kg (11 lbs) within 90 days
• Uncontrolled and potentially unstable diabetic
retinopathy or maculopathy
Research Study of
How Well
Semaglutide Works in
People Living With
Overweight or
Obesity (STEP 7)
Novo Nordisk
NCT04251156
Phase III
MC, QB, PC,
RCT
N~375
Semaglutide 2.4 mg
Placebo
Inclusion Criteria
• Male or female, age ≥18 years
• History of ≥1 unsuccessful dietary effort to lose
body weight
• For subjects without T2DM: BMI ≥30 kg/m
2
or ≥27
kg/m
2
with the ≥1 weight-related comorbidity
(treated or untreated): HTN, dyslipidemia, OSA, or
CVD
• For subjects with T2DM: Treated with either diet
and exercise alone OR stable treatment ≥60 days
with up to 3 oral antidiabetic medications
(metformin, α-glucosidase inhibitor, SU, glinides,
SGLT2i or glitazone), HbA1C 7.0-10.0% (53-86
mmol/mol), BMI ≥27 kg/m
2
Exclusion Criteria
• Change in body weight >5 kg (11 lbs) within 90 days
• For subjects without T2DM at screening: HbA1C
≥6.5% (48 mmol/mol)
• For subjects with T2DM at screening: Renal
impairment measured as eGFR <30 mL/min/1.73
m
2
(<60 mL/min/1.73 m
2
in subjects treated with
SGLT2i)
• Uncontrolled and potentially unstable diabetic
retinopathy or maculopathy
• Change in body
weight [week 0-
44]
• Subjects who
achieve body
weight reduction
equal to or above
5% [week 0-44]
August 2022
Research Study
Looking at How Well
Semaglutide Works in
People Living With
Obesity and
Prediabetes (STEP 10)
Novo Nordisk
Phase III
MC, QB, PC,
RCT
N~201
Semaglutide 2.4 mg
Placebo
Inclusion Criteria
• Male or female aged ≥18 years
• BMI ≥30.0 kg/m
2
• Prediabetes defined as at least one of following:
HbA1C 6-6.4% (42-47 mmol/mol) or FBG 5.5-6.9
mmol/L (99-125 mg/dL)
Exclusion Criteria
•
History of T1DM or T2DM
•
Change in body
weight [week 0-
52]
• Change to
normoglycemia
(normoglycemia
defined as having
both
January
2023

©Institute for Clinical and Economic Review, 2022 Page D85
Evidence Report – Medications for Obesity Management Return to Table of Contents
Title/Trial Sponsor Study Design Treatment Arms Patient Population Primary Outcome(s)
Estimated
Completion
Date
NCT05040971
• Treatment with glucose-lowering agent(s) within 90
days
• HbA1C ≥6.5% (≥48 mmol/mol)
• FPG ≥7.0mmol/L (126 mg/dL)
• Change in body weight >5 kg (11 lbs) within 90 days
• Treatment with any obesity medication within 90
days
HbA1C<6.0%
(<42 mmol/mol)
and FPG <5.5
mmol/L (<99
mg/dL) [week 0-
52]
Research Study
Investigating How
Well Semaglutide
Works in People From
Thailand and South
Korea Living With
Obesity
Novo Nordisk
NCT04998136
Phase III
MC, QB, PC,
RCT
N~150
Semaglutide 2.4 mg
Placebo
Inclusion Criteria:
• Male or female aged ≥18 years
• BMI ≥25 kg/m
2
• Both parents of Asian descent
• History of at least 1 unsuccessful dietary effort to
lose body weight
Exclusion Criteria
• HbA1C at least 48 mmol/mol (6.5%)
• History of T1DM or T2DM
• Change in body weight >5 kg (11 lbs) within 90 days
• Renal impairment with estimated eGFR <15
mL/min/1.73 m
2
at screening
• Change in body
weight [week 0-
44]
• At least 5% body
weight reduction
(yes/no) [week 0-
44]
April 2023
Research Study
Looking at How Well
Semaglutide Works in
People Suffering
From Obesity and
Knee Osteoarthritis
Novo Nordisk
NCT05064735
Phase III
MC, TB, PC,
RCT
N~375
Semaglutide 2.4 mg
Placebo
Inclusion Criteria
• Male or female, age ≥18 years
• BMI ≥30.0 kg/m
2
• Clinical diagnosis of knee OA with moderate
radiographic changes KL grades 2 or 3 as per
central reading) in target (most symptomatic) knee
• Pain due to knee OA
Exclusion Criteria
• Joint replacement in target knee
• Arthroscopy or injections into target knee within
last 3 months prior to enrolment
• Any other joint disease in target knee
• Change in body
weight [week 0-
68]
• Change in
WOMAC pain
score [week 0-
68]
April 2023
Latino Semaglutide
Study (LSS)
Phase III
single-
center, TB,
PC, RCT
Semaglutide 2.4 mg
Placebo
Inclusion Criteria
• Self-identify as being of Hispanic/Latino ethnicity
• BMI >30 kg/m
2
• Age 18-75 years old
• Change from
baseline in
weight loss
[week 0-final
August 2023

©Institute for Clinical and Economic Review, 2022 Page D86
Evidence Report – Medications for Obesity Management Return to Table of Contents
Title/Trial Sponsor Study Design Treatment Arms Patient Population Primary Outcome(s)
Estimated
Completion
Date
Loma Linda University
& Novo Nordisk
NCT05087342
N~375
Exclusion Criteria
• Current cancer treatment
• Diabetes, T1 or T2
• Eating disorders
• Medication use targeting GPL-1 system
• In last 30 days, attempted to lose weight by LSM
alone or with use of anti-obesity medications
resulting in >5 lbs weight loss
• History of bariatric surgery
• Use of obesogenic medications (including but not
limited to steroids, haloperidol, clozapine,
risperidone, olanzapine, amitriptyline, imipramine,
paroxetine, and lithium), which cannot be
substituted or stopped
• Pregnant or planning to become pregnant in next 8
months
• Any contraindication to semaglutide 2.4 mg
including personal or family history of medullary
thyroid carcinoma or multiple endocrine neoplasia
syndrome type 2, hypersensitivity to semaglutide
2.4 mg or any product components
study visit and 7
months post
baseline]
Liraglutide
The Efficacy and
Safety of Liraglutide
on Body Weight Loss
in Obese and
Overweight Patients
Shanghai Zhongshan
Hospital
NCT04605861
Phase III
single-
center, DB,
PC, RCT
N=414
Liraglutide 3 mg
Placebo
Inclusion Criteria
• Aged 18-70 years old
• Failed to control body weight in previous diet
therapy
• Stable body weight (patient reported body weight
change <5 kg) in last 3 months
• BMI ≥30 kg/m
2
(obesity) or BMI ≥27 kg/m
2
(overweight) with ≥1 related metabolic abnormality
(HTN, dyslipidemia, T2DM)
• Those with T2DM: Receiving diet and exercise
therapy alone, or receiving metformin,
sulfonylureas, glycosidase inhibitors and glinides
alone or in combination on basis of diet and
exercise therapy, with their treatment remaining
• % of body weight
loss [week 0-32]
• Proportion of
body weight loss
≥5% [week 0-32]
July 2022

©Institute for Clinical and Economic Review, 2022 Page D87
Evidence Report – Medications for Obesity Management Return to Table of Contents
Title/Trial Sponsor Study Design Treatment Arms Patient Population Primary Outcome(s)
Estimated
Completion
Date
stable, HbA1C 7.0-10.0%, and FBG <13.3 mmol/L
(240 mg/dL)
Exclusion Criteria
• T1DM or secondary DM, acute metabolic
complications; 2 or more severe hypoglycemia
events, binge-eating disorder, hyperthyroidism,
pancreatic cancer, acute gallbladder disease,
psychological disorders, CV and cerebrovascular
diseases, MTC, AIDS, syphilis, proliferative
retinopathy or maculopathy, malignancy
• Receiving GLP-1, DPP-4 inhibitors, SGLT-2 inhibitor,
insulin therapy, OTC weight-loss drugs or appetite
inhibitors, prescription weight-loss drugs, lipid
dissolving infections
• Obesity caused by endocrine diseases
• Taking drugs that can significantly increase weight
in the 3 months
• Previous or planned surgery for obesity
• History of heart valve replacement
• SBP ≥160 mmHg or DBP ≥100 mmHg
• AST or ALT >3.0-fold ULN, or total bilirubin >2.0-
fold ULN
• eGFR <60 mL/min/1.73 m
2
• History of drug abuse
•
Pregnant or breastfeeding
Liraglutide, Phentermine/Topiramate, and Bupropion/Naltrexone
Individualized Obesity
Pharmacotherapy
Mayo Clinic
NCT03374956
Phase III
TB, parallel
assignment,
RCT
N=200
Phenotype-guided
therapy (intervention):
• Phen. 7.5mg/top.
46 mg
• Liraglutide 3 mg
• Bup. 360 mg/nalt.
32 mg
Randomly assigned
therapy (control):
Inclusion Criteria
• Adults with obesity (BMI >30 kg/m
2
)
• No unstable psychiatric disease and controlled
comorbidities or other diseases
• Men or women of childbearing potential with
negative pregnancy tests
Exclusion Criteria
• Abdominal bariatric surgery
• Positive history of chronic GI diseases, or systemic
disease that could affect GI motility, or use of
Total body weight loss
[12 weeks]
July 2022

©Institute for Clinical and Economic Review, 2022 Page D88
Evidence Report – Medications for Obesity Management Return to Table of Contents
Title/Trial Sponsor Study Design Treatment Arms Patient Population Primary Outcome(s)
Estimated
Completion
Date
• Phen. 7.5 mg/top.
46 mg
• Liraglutide 3 mg
• Bup. 360 mg/nalt.
32 mg
• Phen. 15-37.5 mg
medications that may alter GI motility, appetite, or
absorption
• Significant untreated psychiatric dysfunction based
on Hospital Anxiety and Depression Inventory, and
the Questionnaire on Eating and Weight Patterns
(binge eating disorders and bulimia), with anxiety
or depression score >11
AIDS: acquired immunodeficiency syndrome, ALT: alanine aminotransferase, AST: aspartate aminotransferase, BMI: body mass index, CV: cardiovascular, CVD:
cardiovascular disease, DB: double-blind, DBP: diastolic blood pressure, DDP-4: dipeptidyl peptidase 4, dL: deciliter, DM: diabetes mellitus, eGFR: estimated glomerular
filtration rate, FBG: fasting blood glucose, GI: gastrointestinal, GLP-1: glucagon-like peptide 1, HbA1C: glycated hemoglobin, HTN: hypertension, KCCQ: Kansas City
Cardiomyopathy Questionnaire, kg: kilogram, KL: Kellgren and Lawrence, lb: pound, LSM: lifestyle modification, LVEF: left ventricular ejection fraction, m: meter, MC:
multicenter, mg: milligram, MI: myocardial infarction, min: minute, mmol/mol: millimoles per mole, mmol/L: millimoles per liter, mL: milliliter, MTC: medullary thyroid
cancer, N: total number, NYHA: New York Heart Association, OA: osteoarthritis, OSA: obstructive sleep apnea, OTC: over the counter, PAD: peripheral artery disease,
PC: placebo-controlled, QB: quadruple blind, RCT: randomized controlled trial, SBP: systolic blood pressure, SGLT2: sodium-glucose co-transporter-2, SU: sulphonylurea,
TB: triple-blind, ULN: upper limits of normal, WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index
Source: www.ClinicalTrials.gov
(NOTE: studies listed on site include both clinical trials and observational studies).

©Institute for Clinical and Economic Review, 2022 Page D89
Evidence Report – Medications for Obesity Management Return to Table of Contents
D5. Previous Systematic Reviews and Technology Assessments
We identified 15 systematic literature reviews or meta-analyses evaluating therapies for weight-loss
treatment in adults with overweight or obesity, two of which are summarized below.
Shi, Q., et al. (2022). “Pharmacotherapy for Adults with Overweight and Obesity: A Systematic
Review and Network Meta-Analysis of Randomised Controlled Trials”
95
This systematic review and network meta-analysis evaluated the comparative efficacy and safety of
several medications for adults with overweight and obesity who were seeking weight-loss
management. The interventions assessed included semaglutide, liraglutide,
phentermine/topiramate, bupropion/naltrexone, metformin, orlistat, exenatide, pramlintide,
dapagliflozin, empagliflozin, canagliflozin, ertugliflozin, ipragliflozin/metformin/pioglitazone, and
sibutramine/levocarnitine. Inclusion criteria included randomized controlled trials evaluating a
candidate weight-lowering drug in comparison to placebo, lifestyle modification, or an alternative
drug. Studies were excluded if their outcomes did not focus on weight loss or quality of life
measures and if they recruited patients with psychological disorders and eating disorders. Search
terms for PubMed, Embase, and Cochrane Library searches included “weight loss,” “weight-loss
drugs,” and “RCTs.” By March 2021, investigators identified 143 randomized controlled trials
(N=49,810) for inclusion. Median age was 47, the proportion of females was 75%, median BMI was
35.3, and median duration of follow-up was 24 weeks. Data on the GLP-1 receptor agonists
(semaglutide, liraglutide, and exenatide) were presented together.
Phentermine/topiramate (MD: -7.97; 95% CI: -9.28 to -6.66) and the GLP-1 receptor agonists (MD:
5.76; 95% CI: -6.30 to -5.21) were the most effective at helping participants achieve percentage and
absolute body weight change from baseline, and all drugs except levocarnitine were associated with
a reduction in body weight. For the categorical outcome of weight loss of at least 5% or 10% body
weight, phentermine/topiramate, GLP-1 receptor agonists, and bupropion/naltrexone were the
most effective at helping participants achieve these categorical outcomes, and more than doubled
the proportion of participants receiving these interventions losing at least 5% or 10% body weight
compared to participants who were receiving lifestyle modification alone. In post-hoc analyses,
semaglutide (separate from the other GLP-1 agonists) demonstrated the largest percent weight loss
(MD: -11.41; 95% CI: -12.54 to -10.27) and had the highest likelihood of achieving target weight loss
of at least 5% and 10%. In terms of subgroup effects, participants receiving GLP-1 receptor agonists
achieved a greater amount of weight loss if they were non-diabetic, compared to participants who
had diabetes. However, this has low credibility due to inconsistency across studies.
Quality-of-life outcomes were available in 15 trials that looked at health-related quality of life
scores, and in seven trials that assessed depression, and included the drugs
phentermine/topiramate, bupropion/naltrexone, GLP-1 receptor agonists, and orlistat. All drugs in
this network except orlistat helped improve quality of life, improvements in depression scores from

©Institute for Clinical and Economic Review, 2022 Page D90
Evidence Report – Medications for Obesity Management Return to Table of Contents
baseline were not statistically significant. For secondary outcomes, GLP-1 receptor agonists
significantly reduced HbA1C levels when compared to lifestyle modification alone, and orlistat
significantly reduced LDL cholesterol compared to lifestyle modification. GLP-1 receptor agonists
and phentermine/topiramate were associated with the largest reductions in systolic blood pressure.
With regards to safety, phentermine/topiramate, bupropion/naltrexone, GLP-1 receptor agonists,
and orlistat were associated with an increased risk of participants discontinuing due to adverse
events. Between the drugs, bupropion/naltrexone and phentermine/topiramate were found to
have the most discontinuations due to adverse events.
Investigators concluded that phentermine/topiramate and GLP-1 receptor agonists were most
effective for weight loss, with high to moderate certainty of evidence, and demonstrated small
benefits on quality-of-life outcomes. Evidence on other secondary outcomes were of low to very
low certainty. Limitations included the lack of individual patient data pooling, which prevented
more precise subgroup analyses, and heterogeneity in participant baseline characteristics and
duration of follow-up.
Arastu, N., et al. (2022). “Efficacy of Subcutaneous Semaglutide Compared to Placebo for Weight
Loss in Obese, Non-Diabetic Adults: A Systematic Review & Meta-Analysis”
150
Investigators conducted a systematic review and meta-analysis evaluating the efficacy of
subcutaneous semaglutide in treating obesity in adults with overweight or obesity without
diabetes, compared to placebo. Randomized controlled trials of adult participants with a BMI ≥27
kg/m
2
were included, and studies that included participants who were under 18 years of age or had
type 1 or type 2 diabetes mellitus were excluded. EBSCOhost (including CINAHL Complete,
Academic search Premier, MEDLINE, and Cochrane Central Register of Controlled Trials) was used
for the literature search and included search terms such as “semaglutide,” “Wegovy,” “obesity,”
and “overweight.” By August 31, 2021, investigators identified four studies (N=2,882) that met
eligibility criteria and were included in quantitative synthesis. The mean age was 46 years. All
studies were determined to have low risks of bias.
For the primary outcome of mean body weight loss, the mean difference of weight loss in
participants receiving semaglutide versus placebo was -11.62 kg (95% CI: -13.03 to -10.21;
p<0.00001), indicating that semaglutide demonstrated a statistically significant reduction in weight
loss compared to placebo. Additionally, the proportion of participants receiving semaglutide, who
achieved weight loss of at least 5% was higher in all trials compared to placebo (p<0.001).
Semaglutide was also associated with a statistically significant reduction in waist circumference
(MD: -9.16 cm; 95% CI: -9.91 to -8.40; p<0.00001), and BMI (MD: -4.33 kg/m2; 95% CI: -4.88 to -
3.78; p<0.00001). Subgroup analyses between the semaglutide 2.4 mg dose and the 0.4 mg dose
indicated no significant differences between the treatment doses.

©Institute for Clinical and Economic Review, 2022 Page D91
Evidence Report – Medications for Obesity Management Return to Table of Contents
While semaglutide was shown to be superior to placebo in helping reduce body weight in
participants with overweight or obesity, investigators identified several potential limitations,
including the limited number of studies, variability in type of lifestyle modification, and lack of long-
term data on semaglutide.

©Institute for Clinical and Economic Review, 2022 Page E1
Evidence Report – Medications for Obesity Management Return to Table of Contents
E. Long-Term Cost-Effectiveness: Supplemental
Information
E1. Methods
Rationale for Not Including Certain Health States in the Base Case
We did not include cancer, osteoarthritis, joint surgery, or sleep apnea as separate Markov states in
our model because: 1) the causal association between weight reduction and decreasing the
incidence of cancer or osteoarthritis is uncertain, 2) any benefits of modest weight loss on cancer
and osteoarthritis are estimated to be small relative to the cardiovascular benefits being assessed,
3) the impact of any improvement on cardiovascular outcomes from improvements in sleep apnea
associated with weight loss would be captured from the changes in weight loss- and blood
pressure-related cardiovascular disease and mortality, 4) the cost of treating sleep apnea, such as a
continuous positive airway pressure machine, would have a negligible impact on the incremental
cost, 5) the short-term impact of weight loss on quality of life due to sleep apnea is inherently
included as a utility gain associated with weight loss, measured directly in clinical trials but not
explicitly stated as resulting from changes to sleep apnea, and 6) there is no known evidence from
semaglutide trials or other pharmacotherapy clinical trials demonstrating that these therapies
directly reduce the risk of or morbidity associated with weight-related comorbidities.
Impact Inventory
Consistent with the recommendations from the Second Panel on Cost Effectiveness in Health and
Medicine, the impact inventory of what was included in the base case and scenario analyses from
the health care sector and societal perspectives, respectively, is shown in Table E1.
151

©Institute for Clinical and Economic Review, 2022 Page E2
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table E1. Impact Inventory
Sector
Type of Impact (Add Additional
Domains, as Relevant)
Included in This Analysis
from […] Perspective?
Notes on Sources (if
Quantified), Likely Magnitude
& Impact (if Not)
Health Care
Sector
Societal
Formal Health Care Sector
Health
Outcomes
Longevity effects
X
X
HRQoL effects
X
X
Adverse events
Evaluated, but did not include
AEs. Expected that AEs would
lead to treatment disc. early in
therapy and not to significant
costs or disutility.
Medical Costs
Paid by third-party payers
X
X
Paid by patients out-of-pocket Possibly Possibly
Sources used for cost estimates
provided comprehensive
descriptions for what medical
costs were included, but did not
include whether out-of-pocket
costs were included in
estimates.
Future related medical costs
X
X
Future unrelated medical costs
Informal Health Care Sector
Health-Related
Costs
Patient time costs
N/A
Unpaid caregiver-time costs
N/A
Transportation costs
N/A
Non-Health Care Sector
Productivity
Labor market earnings lost
N/A
X
Cost of unpaid lost productivity
due to illness
N/A X
Cost of uncompensated
household production
N/A
Consumption
Future consumption unrelated to
health
N/A
Social Services
Cost of social services as part of
intervention
N/A
Legal/Criminal
Justice
Number of crimes related to
intervention
N/A
Cost of crimes related to
intervention
N/A
Education
Impact of intervention on
educational achievement of
population
N/A
Housing
Cost of home improvements,
remediation
N/A
Environment
Production of toxic waste
pollution by intervention
N/A
Other
Other impacts (if relevant)
N/A
AE: adverse event, N/A: not applicable
Adapted from Sanders et al.
151

©Institute for Clinical and Economic Review, 2022 Page E3
Evidence Report – Medications for Obesity Management Return to Table of Contents
Description of evLY Calculations
The evLY considers any extension of life at the same “weight” no matter what treatment is being
evaluated or what population is being modeled. Below are the stepwise calculations used to
calculate the evLY.
1) First, we attribute a utility of 0.851, the age- and sex-adjusted utility of the general
population in the US that are considered healthy.
152
2) We calculate the evLY for each model cycle.
3) Within a model cycle, if using the intervention results in additional life years versus the
primary comparator, we multiply the general population utility of 0.851 with the
additional life years gained (ΔLY gained) within the cycle.
4) The life years shared between the intervention and the comparator use the
conventional utility estimate for those life years within the cycle.
5) The total evLY for a cycle is calculated by summing steps 3 and 4.
6) The evLY for the comparator arm is equivalent to the QALY for each model cycle.
7) The total evLYs are then calculated as the sum of evLYs across all model cycles over the
time horizon.
Finally, the evLYs gained is the incremental difference in evLYs between the intervention and the
comparator arm.
Target Population
Model inputs were chosen based upon patient characteristics in clinical trials. Patient age, BMI,
gender, SBP, smoking status, and presence of hypertension and diabetes mellitus were required
inputs for calculating mortality and cardiovascular risk. Consistent with clinical trials and real-world
evidence on users of medications for weight management, patients were 80% female with average
age of 45 years, BMI of 38 kg/m
2
, SBP of 125 mmHg, and HbA1C of 5.5% at model entry.
33,43,53,56,61,83
The base-case model cohort characteristics are shown in Table E2.
Table E2. Base-Case Model Cohort Characteristics
Value
Primary Sources
Mean Age
45 years
CONQUER, EQUIP, COR-I, SCALE,
STEP 1, STEP 8
33,43,53,56,61,83
Mean BMI
38 kg/m
2
Female
80.0%
Mean SBP
125 mmHg
Diagnosis of Hypertension
(Actively Treated)
35.0%
Diagnosis of Diabetes Mellitus
0%
Assumption for base case
Smoking
12.5%
CDC
153
CDC: Centers for Disease Control and Prevention, BMI: body mass index, kg: kilogram, m: meter, mmHg: millimeter
of mercury, SBP: systolic blood pressure

©Institute for Clinical and Economic Review, 2022 Page E4
Evidence Report – Medications for Obesity Management Return to Table of Contents
Treatment Strategies
• Semaglutide
o Titration: 0.25 mg administered subcutaneously once weekly for the first four
weeks, with the dose increased every four weeks to reach the maintenance dose of
2.4 mg by week 16
o Maintenance dose: 2.4 mg administered subcutaneously once a week
• Liraglutide
o Titration: Starting at a dose of 0.6 mg with weekly 0.6-mg increments to 3.0 mg
o Maintenance dose: 3.0 mg administered subcutaneously once daily
• Phentermine/topiramate extended-release
o Loading dose: 3.75 mg/23 mg (phentermine 3.75 mg/topiramate 23 mg ER) daily for
14 days; then increase to the maintenance dose 1 and 2. Maintenance dose 2 is the
target regimen of our study.
o Maintenance dose 1: 7.5 mg/46 mg daily
o Maintenance dose 2: 15 mg/92 mg daily
• Bupropion/naltrexone ER
o Titration: Starting at a dose of 8 mg/90 mg once a day for a week, with weekly
increases in 8 mg/90 mg increments until dose of 16 mg/180 mg twice daily is
achieved at week four
o Maintenance dose: 16 mg/180 mg twice daily (32 mg/360 mg per day)
E2. Model Inputs and Assumptions
Key model assumptions and rationales are presented in Table 4.1 of the Report. Additional model
assumptions/rationales are listed in Table E3 below.

©Institute for Clinical and Economic Review, 2022 Page E5
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table E3. Model Assumptions
Assumption
Rationale
Proportion of smokers does
not vary over time
Smoking behavior has not been convincingly shown to be influenced by
FDA-approved anti-obesity interventions. However, we do acknowledge
that despite it not being a comparator or intervention in the base-case
analysis, bupropion alone (Zyban®, GlaxoSmithKline) is approved for
smoking cessation. This assumption may therefore result in an
underestimation of bupropion’s effect on cardiovascular events.
Inclusion of adverse events in
the model would add
significant complexity without
providing much improvement
in cost-effectiveness
estimation or face validity to
the model
Adverse events reported with these four medications occur early, are
generally not severe in nature, and would normally not lead to appreciable
treatment discontinuation as compared to inadequate weight loss
response. However, we adjusted the cost of treatment by the probability
of discontinuation to estimate the impact of early treatment
discontinuation due to adverse events or lack of effectiveness.
Once patients develop diabetes
mellitus, their diabetes care
and associated diabetes
outcomes is similar between
those who are on weight
management and those who
are not
Although liraglutide and semaglutide affect blood glucose, the treatment
pathways for diabetes mellitus in those who will have access to liraglutide
and semaglutide would also include access to these treatments for
diabetes mellitus, albeit potentially at a different dose. We assumed that
diabetes treatment outcomes would not differ in patients with treatments
that affect HbA1C versus those that did not.
FDA: Food and Drug Administration, HbA1C: glycated hemoglobin, SBP: systolic blood pressure
Model Inputs
Clinical Inputs
The key model inputs are listed in Table 4.2 of the Report. Those inputs, plus additional inputs, are
listed in Table E4 below.

©Institute for Clinical and Economic Review, 2022 Page E6
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table E4. Key Model Inputs
Parameter
Input
Source
Clinical Inputs
Absolute Difference in % Weight Change, SEM vs. LSM
-13.7%
ICER NMA, Table 3.11
Absolute Difference in HbA1C Change, SEM vs. LSM
-0.30
STEP 1
83
Absolute Difference in % Weight Change, LIR vs. LSM
-5.0%
ICER NMA, Table 3.11
Absolute Difference in HbA1C Change, LIR vs. LSM
-0.20
SCALE (Maintenance)
84
Absolute Difference in % Weight Change, P/T vs. LSM
-9.1%
ICER NMA, Table 3.11
Absolute Difference in HbA1C Change, P/T vs. LSM
0.00
EQUIP
53,56
Absolute Difference in % Weight Change, B/N vs. LSM
-4.6%
ICER NMA, Table 3.11
Absolute Difference in HbA1C Change, B/N vs. LSM
0.00
61,65
Treatment Discontinuation, SEM
0.042
ICER NMA, Table 3.19
Treatment Discontinuation, LIR
0.058
ICER NMA, Table 3.19
Treatment Discontinuation, P/T
0.058
ICER NMA, Table 3.19
Treatment Discontinuation, B/N
0.053
ICER NMA, Table 3.19
Treatment Discontinuation, LSM
0.025
STEP 1, STEP 2, STEP 4, STEP 6
Baseline Risk of CV Event, Female Non-Smoker without Treated
HTN
0.04
Framingham Risk Calculation
Coefficient
88
Baseline Risk of CV Event, Male Smoker with Treated HTN
0.23
Multiplier for Probability of MI from CV Risk
0.22
Multiplier for Probability of Stroke from CV Risk
0.23
Multiplier for Probability of Other CVD from CV Risk
0.55
Probability of Mortality Following Acute MI
0.08
OECD Statistics
154
Probability of Mortality Following Acute Stroke
0.08
Relative Risk of Annual Mortality Post-MI
1.58
Majed 2015
82
Relative Risk of Annual Mortality Post-Stroke
3.13
Relative Risk of Annual Mortality with Other CVD
1.9
Pande 2011
80
Relative Risk of Annual Mortality Post-HF
1.82
Ødegaard 2020
81
Relative Risk of Annual Mortality Post-DM
1.15
Tancredi 2015
79
Annual Probability of Recurrent MI in Male
0.0813
Peters 2021
155
Annual Probability of Recurrent MI in Female
0.0723
Annual Probability of Recurrent Stroke
0.12
Kolmos 2021
156
Proportion of Male Patients with Hypertension, BMI <25
0.14
Wang 2004
157
Proportion of Female Patients with Hypertension, BMI <25
0.164
Proportion of Male Patients with Hypertension, BMI ≥25 to 30
0.268
Proportion of Female Patients with Hypertension, BMI ≥25 to 30
0.292
Proportion of Male Patients with Hypertension, BMI ≥30
0.431
Proportion of Female Patients with Hypertension, BMI ≥30
0.42
Probability of Developing HF from Acute MI, Age 25-54
0.0994
Sulo 2016
94
Probability of Developing HF from Acute MI, Age 55-74
0.1648
Probability of Developing HF from Acute MI, Age 75-85
0.268
Annual probability of Developing HF Post MI, Age 25-54
0.012
Annual probability of Developing HF Post MI, Age 55-74
0.031
Annual probability of Developing HF Post MI, Age 75-85
0.080
Comorbidity Cost Inputs
Cost Other CVD
$14,279
Scully 2017
97
Cost Acute Stroke
$17,316
HCUP
98
Cost Post Stroke
$6,500
Kazi 2019
99
Cost Acute MI
$26,034
HCUP
98
Cost Post MI
$3,117
Kazi 2016
100
Cost HF, First Year
$27,030
Patel 2021
101
; Urbich 2020
102
Cost HF, Second Year or Later
$15,605
Patel 2021
101
©Institute for Clinical and Economic Review, 2022 Page E7
Evidence Report – Medications for Obesity Management Return to Table of Contents
Parameter
Input
Source
Cost DM
$11,425
ADA 2018
103
Risk Equations
Onset of Cardiovascular Condition, 10-Year Risk
Office-Based Non-Laboratory Prediction Model
Baseline and Beta Coefficient
Women
Men
So(10)
0.94833
0.8843
Log of Age
2.72107
3.113
BMI
0.51125
0.7928
Log of SBP if not treated
2.81291
1.8551
Log of SBP if treated
2.88267
1.9267
Smoking
0.61868
0.7095
Diabetes
0.77763
0.5316
Framingham Risk Calculation
Coefficient
88
Onset of Diabetes, Annual Risk
1.46×10
-6
exp (1.87×HbA1C) × 1.97×10
-2
exp (0.101×BMI)
Exponential regression from
Edelman et al.
85
BMI: body mass index, B/N: bupropion/naltrexone, CV: cardiovascular, CVD: cardiovascular disease, DM: diabetes
mellitus, HbA1C: glycated hemoglobin, HF: heart failure, HTN: hypertension, ICER: Institute for Clinical and Economic
Review, LIR: liraglutide, LSM: lifestyle modification, NMA: network meta-analysis, P/T: phentermine/topiramate, SEM:
semaglutide
Clinical Probabilities/Response to Treatment
Response to treatment was determined from clinical trials evaluating drug treatments plus lifestyle
modification versus lifestyle modification alone or compared with other treatments, where such
studies existed.
33,53,56,61,83,84
The primary outcome evaluated for this model was weight change
relative to the comparator, evaluated using the NMA depicted in Table 3.11 of the Report. Patients
would achieve the maximum weight reduction before the end of year one and maintained the
maximum efficacy while the initial treatment is maintained. A secondary outcome, needed for
determining the proportion of people developing diabetes mellitus each cycle, was mean reduction
in HbA1C.
Mortality
For patients without pre-existing comorbidities, mortality was estimated from age- and gender-
adjusted mortality rates in the general population, using all-cause mortality from the Human
Mortality Database US-specific tables.
96
This mortality probability was multiplied by the relative risk
for mortality for each post-event state, specifically post-myocardial infarction, post-stroke, other
cardiovascular disease, and heart failure.
79-82
In addition, mortality from the acute myocardial
infarction and acute stroke events was also factored into the model.
154

©Institute for Clinical and Economic Review, 2022 Page E8
Evidence Report – Medications for Obesity Management Return to Table of Contents
Adverse Events
Adverse events were not considered in the model, as adverse events of weight loss medications
were unlikely to generate measurable health care costs or health utility losses. However, in
calculating average treatment effect, patients who discontinue the treatment due to an adverse
event were assumed to be a part of the study cohort. Cost of treatment was adjusted for the
proportion of patients who continue treatment where the treatment discontinuation was assumed
to incur at the very beginning of the first model cycle. Discontinuation rates were calculated from
the NMA results. (Table 3.19)
Economic Inputs
Administration and Monitoring Costs
Administration costs were determined to be nominal for these injectable and oral products, which
are administered at home. The injectable products, semaglutide and liraglutide, are dispensed as
single-use subcutaneous injection pens. Monitoring costs were also determined to be nominal and
were not included in the model. Table E5 presents the dose, frequency, and route of administration
as well as monitoring and administration utilization of each intervention.
Table E5. Dose, Frequency of Administration, and Annual Monitoring and Administration
Utilization
Intervention
Route
Dose
Frequency of Administration
Semaglutide
Subcutaneous
2.4 mg
Weekly
Liraglutide
Subcutaneous
3 mg
Daily
Phentermine/
Topiramate
Oral 15 mg/92 mg
Daily
Bupropion/
Naltrexone
Oral 32 mg/360 mg Daily
mg: milligram

©Institute for Clinical and Economic Review, 2022 Page E9
Evidence Report – Medications for Obesity Management Return to Table of Contents
E3. Results
Cost-Effectiveness Plane
Figure E1 presents the cost-effectiveness plane. The x-axis represents therapy benefit and the y-
axis represents cost. Each point in the plane represents the estimated cost and effectiveness in the
base-case result for a particular therapy option added to lifestyle modification.
Figure E1. Cost-Effectiveness Plane
B/N: bupropion/naltrexone, LIR: liraglutide, LSM: lifestyle management, P/T: phentermine/topiramate, QALY:
quality-adjusted life year, SEM: semaglutide, USD: United States Dollar
SEM
LIR
P/T
B/N
LSM
$0
$100,000
$200,000
$300,000
$400,000
$500,000
16.50 17.00 17.50 18.00
Discounted Cost (USD)
Discounted QALY gained

©Institute for Clinical and Economic Review, 2022 Page E10
Evidence Report – Medications for Obesity Management Return to Table of Contents
Undiscounted Base-Case Results
Discounted base-case results and incremental results are presented in Report Tables 4.4 and 4.5.
The undiscounted base-case results are presented in Table E6. The undiscounted incremental
results compared to lifestyle modification are shown in Table E7.
Table E6. Undiscounted Base-Case Results
Treatment Drug Cost Non-Drug Cost Total Cost
Life
Years
QALYs evLYs
Semaglutide
$463,900
$213,800
$677,700
34.14
28.73
28.76
Liraglutide
$390,100
$267,300
$657,400
33.64
27.73
27.76
Phentermine/Topiramate
$64,100
$281,400
$345,500
33.62
27.78
27.81
Bupropion/Naltrexone
$84,000
$302,700
$386,600
33.40
27.35
27.36
Lifestyle Modification*
$18,300
$324,200
$342,400
33.19
26.91
26.91
evLY: equal-value life year, QALY: quality-adjusted life year
*Reference for evLY calculation for all active treatments.
Table E7. Undiscounted Incremental Results for the Base Case
Incremental Values vs. Lifestyle Modification
Treatment Drug Cost
Non-Drug
Cost
Total Cost
Life
Years
QALYs evLYs
Semaglutide
$445,600
-$110,400
$335,300
0.95
1.82
1.85
Liraglutide
$371,800
-$56,900
$315,000
0.45
0.82
0.85
Phentermine/Topiramate
$45,800
-$42,800
$3,100
0.42
0.88
0.90
Bupropion/Naltrexone
$65,700
-$21,500
$44,200
0.21
0.44
0.45
Lifestyle Modification*
--
--
--
--
--
--
evLY: equal-value life year, QALY: quality-adjusted life year
*Reference for incremental calculation for all active treatments.
Key incremental cost per QALY ratios over the lifetime horizon are shown in Table 4.6 of the Report
for each of the treatment strategies. All calculated incremental ratios over the lifetime horizon
between treatment options included in our model are show in Table E8.

©Institute for Clinical and Economic Review, 2022 Page E11
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table E8. Incremental Cost-Effectiveness Ratios for the Base Case, Results from Discounted and
Undiscounted Outcomes
Treatment Comparator
Cost per Life
Year Gained
Cost per QALY
Gained
Cost per evLY
Gained
Discounted Results
Semaglutide
Lifestyle modification
$624,000
$238,000
$235,000
Liraglutide
Lifestyle modification
$1,210,000
$485,000
$475,000
Phentermine/Topiramate
Lifestyle modification
$22,000
$8,000
$7,000
Bupropion/Naltrexone
Lifestyle modification
$359,000
$124,000
$121,000
Semaglutide
Liraglutide
$85,000
$31,000
$31,000
Phentermine/topiramate
$1,128,000
$472,000
$468,000
Bupropion/naltrexone
$703,000
$277,000
$274,000
Liraglutide
Phentermine/topiramate $23,837,000
P/T less costly,
more effective
P/T less costly,
more effective
Bupropion/naltrexone
$1,991,000
$941,000
$921,000
Phentermine/Topiramate Bupropion/naltrexone
P/T less costly,
more effective
P/T less costly,
more effective
P/T less costly,
more effective
Undiscounted Results
Semaglutide
Lifestyle modification
$352,000
$184,000
$181,000
Liraglutide
Lifestyle modification
$702,000
$382,000
$371,000
Phentermine/Topiramate
Lifestyle modification
$7,000
$4,000
$3,000
Bupropion/Naltrexone
Lifestyle modification
$209,000
$101,000
$98,000
Semaglutide
Liraglutide
$40,000
$20,000
$20,000
Phentermine/topiramate
$630,000
$352,000
$348,000
Bupropion/naltrexone
$394,000
$211,000
$208,000
Liraglutide
Phentermine/topiramate
$12,807,000
P/T less costly,
more effective
P/T less costly,
more effective
Bupropion/naltrexone
$1,145,000
$702,000
$681,000
Phentermine/Topiramate Bupropion/naltrexone
P/T less costly,
more effective
P/T less costly,
more effective
P/T less costly,
more effective
evLY: equal-value life year, PT: phentermine/topiramate, QALY: quality-adjusted life year
Cumulative Incidence of Cardiovascular Conditions and Mortality
Average life expectancy in patients receiving semaglutide and lifestyle modification was 34.14 and
33.19 years, respectively. The respective cumulative incidence of any major cardiovascular
condition through the end of the model time horizon was 52.06% and 59.51%. Figures E2 and E3
present the overall survival estimates and cumulative incidence of cardiovascular conditions across
the five treatment arms.

©Institute for Clinical and Economic Review, 2022 Page E12
Evidence Report – Medications for Obesity Management Return to Table of Contents
Figure E2. Cumulative Incidence of Any Major Cardiovascular Comorbidity
B/N: bupropion/naltrexone, LIR: liraglutide, LSM: lifestyle modification, P/T: phentermine/topiramate, SEM:
semaglutide
Figure E3. Overall Survival
B/N: bupropion/naltrexone, LIR: liraglutide, LSM: lifestyle modification, P/T: phentermine/topiramate, SEM:
semaglutide
0%
20%
40%
60%
80%
100%
45 50 55 60 65 70 75 80 85 90 95 100
Cumulative Incidence
Age (year)
SEM
LIR
P/T
B/N
LSM
0%
20%
40%
60%
80%
100%
45 50 55 60 65 70 75 80 85 90 95 100
Overall Survival
Age (year)
SEM
LIR
P/T
B/N
LSM

©Institute for Clinical and Economic Review, 2022 Page E13
Evidence Report – Medications for Obesity Management Return to Table of Contents
E4. Sensitivity Analyses
One-Way Sensitivity Analysis
The model was sensitive to several inputs, including the disutility per BMI change, baseline HbA1C,
cost of diabetes mellitus management, baseline BMI, weight-lowering effect of treatment
compared to lifestyle management, and change in HbA1C with treatment. The one-way sensitivity
analysis results and tornado diagrams for each treatment option are presented in Table E9 on the
following page.

©Institute for Clinical and Economic Review, 2022 Page E14
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table E9. Tornado Diagram Inputs and Results for One-Way Sensitivity Analyses (by Incremental Cost-Effectiveness Ratio)†
SEM vs. LSM
Input Variable
Lower Input
Higher Input
Lower Input ICER
Higher Input ICER
Disutility per BMI change
-0.00555
-0.00111
$197,000
$301,000
Baseline HbA1C
5.1
5.85
$230,000
$325,000
Cost of DM
$7,501
$17,418
$206,000
$259,000
Baseline BMI
35
40
$222,000
$272,000
Difference in % Weight Change, SEM vs. LSM
-0.14974
-0.12466
$221,000
$258,000
Difference in HbA1C between SEM and LSM
-0.33018
-0.26982
$231,000
$246,000
Relative Risk of Mortality for Other CVD
1.3
2.8
$231,000
$244,000
Relative Risk of Mortality for Stroke
1.98
4.92
$233,000
$244,000
SEM Treatment Discontinuation Rate
0.032
0.054
$234,000
$241,000
Age-Related Disutility
-0.0009
-0.0005
$235,000
$241,000
Probability of Stroke Occurring in Those with CV
0.18793
0.274094
$236,000
$240,000
Relative Risk of Mortality for MI
1.18
2.12
$236,000
$240,000
Relative Risk of Mortality for DM
1.14
1.16
$236,000
$240,000
Proportion Female
0.741
0.817504
$236,000
$239,000
Cost of Other CVD
$10,056
$18,498
$237,000
$239,000
Probability of Mortality for Acute MI
0.05274
0.098482
$237,000
$239,000
Annual Weight Gain
0
0.004
$238,000
$240,000
Probability of Mortality for Acute Stroke
0.05605
0.102826
$237,000
$239,000
Proportion of CV Events that are MIs
0.18032
0.265386
$237,000
$239,000
Cost of HF, Second Year or Later
$10,098
$24,115
$237,000
$238,000
LRG vs. LSM
Input Variable
Lower Input
Higher Input
Lower Input ICER
Higher Input ICER
Disutility per BMI change
-0.00555
-0.00111
$419,000
$576,000
Baseline HbA1C
5.1
5.85
$484,000
$628,000
Difference in % Weight Change, LIR vs. LSM
-0.061
-0.039
$423,000
$567,000
Difference in HbA1C between LIR and LSM
-0.23018
-0.16982
$453,000
$522,000
Baseline BMI
35
40
$469,000
$531,000
Cost of DM
$7,501
$17,418
$448,000
$510,000
Relative Risk of Mortality for Other CVD
1.3
2.8
$470,000
$499,000
Relative Risk of Mortality for Stroke
1.98
4.92
$473,000
$499,000
Age-Related Disutility
-0.0009
-0.0005
$479,000
$493,000
Annual Weight Gain
0
0.004
$485,000
$499,000
LIR Treatment Discontinuation Rate
0.049
0.067
$479,000
$491,000
Probability of Stroke Occurring in Those with CV
0.18793
0.274094
$481,000
$490,000
Relative Risk of Mortality for MI
1.18
2.12
$481,000
$490,000
Relative Risk of Mortality for DM
1.14
1.16
$482,000
$489,000
Proportion Female
0.741
0.817504
$481,000
$487,000
Probability of Mortality for Acute MI
0.05274
0.098482
$484,000
$487,000
Probability of Mortality for Acute Stroke
0.05605
0.102826
$484,000
$487,000
Baseline Age
44.4246
45.57539
$485,000
$487,000
Proportion of CV events that are MIs
0.18032
0.265386
$484,000
$487,000
Cost of Other CVD
$10,056
$18,498
$484,000
$487,000
$175,000 $200,000 $225,000 $250,000 $275,000 $300,000 $325,000
$400,000 $450,000 $500,000 $550,000 $600,000 $650,000

©Institute for Clinical and Economic Review, 2022 Page E15
Evidence Report – Medications for Obesity Management Return to Table of Contents
P/T vs. LSM
Input Variable
Lower Input
Higher Input
Lower Input ICER
Higher Input ICER
Cost of DM
$7,501
$17,418
$24,000
-$17,000
Difference in % Weight Change, P/T vs. LSM
-0.111
-0.0715
-$3,000
$24,000
Baseline HbA1C
5.1
5.85
$26,000
$7,000
Baseline BMI
35
40
$16,000
$4,000
Difference in HbA1C between B/N and LSM
-0.030184
0.030184
$1,000
$9,000
Disutility per BMI Change
-0.00555
-0.00111
$6,000
$11,000
P/T Treatment Discontinuation Rate
0.040
0.081
$9,000
$5,000
Cost of Other CVD
$10,056
$18,498
$9,000
$6,000
Annual Weight Gain
0
0.004
$8,000
$9,000
Cost of HF, Second Year or Later
$10,098
$24,115
$7,000
$8,000
Relative Risk of Mortality for Other CVD
1.3
2.8
$8,000
$7,000
Relative Risk of Mortality for Stroke
1.98
4.92
$7,000
$8,000
Cost of Acute MI
$16,462
$41,171
$8,000
$7,000
Cost of Acute Stroke
$11,153
$26,886
$8,000
$7,000
Proportion of CV Events that are Strokes
0.188
0.274
$7,000
$8,000
LSM Treatment Discontinuation Rate
0.017
0.035
$7,000
$8,000
Cost of Post Stroke
$5,418
$7,801
$8,000
$7,000
Proportion Female
0.741
0.818
$7,000
$8,000
Relative Risk of Mortality for MI
1.18
2.12
$7,000
$8,000
Age-Related Disutility
-0.0009
-0.0005
$8,000
$7,000
B/N vs. LSM
Input Variable
Lower Input
Higher Input
Lower Input ICER
Higher Input ICER
Difference in % Weight Change, B/N vs. LSM
-0.0604
-0.0311
$81,000
$210,000
Disutility per BMI Change
-0.00555
-0.00111
$97,000
$172,000
Cost of DM
$7,501
$17,418
$140,000
$99,000
Baseline HbA1C
5.1
5.85
$153,000
$125,000
Difference in HbA1C between B/N and LSM
-0.13872
-0.11128
$100,000
$129,000
Baseline BMI
35
40
$142,000
$116,000
B/N Treatment Discontinuation Rate
0.036
0.073
$128,000
$119,000
Relative Risk of Mortality for Other CVD
1.3
2.8
$127,000
$120,000
Relative Risk of Mortality for Stroke
1.98
4.92
$127,000
$121,000
Annual weight gain
0
0.004
$124,000
$129,000
Age-Related Disutility
-0.0009
-0.0005
$126,000
$122,000
Cost of Other CVD
$10,056
$18,498
$125,000
$122,000
Probability of Stroke Occurring in Those with CV
0.18793
0.274094
$125,000
$123,000
Relative Risk of Mortality for MI
1.18
2.12
$125,000
$123,000
Proportion Female
0.741
0.818
$122,000
$124,000
Relative Risk of Mortality for DM
1.14
1.16
$124,000
$123,000
Cost of HF, Second Year or Later
$10,098
$24,115
$124,000
$123,000
LSM Treatment Discontinuation Rate
0.017
0.027
$123,000
$124,000
Relative Risk of Mortality for MI
1.18
2.12
$124,000
$123,000
Baseline Age
44.4246
45.57539
$124,000
$123,000
BMI: body mass index, B/N: bupropion/naltrexone, CV: cardiovascular, CVD: cardiovascular disease, DM: diabetes mellitus, Hb: hemoglobin, HF: heart failure, ICER: incremental cost-effectiveness ratio, LIR: liraglutide, LSM: lifestyle modification, MI: myocardial
infarction, P/T: phentermine/topiramate, SEM: semaglutide
*Note lower input may reflect either upper or lower ICER value depending on the direction that the input has on the ICER output. †In the tornado diagram, blue bars denote effects from low input estimates, while green bars denote effects from high input estimates.
-$20,000 -$10,000 $0 $10,000 $20,000 $30,000
$50,000 $100,000 $150,000 $200,000 $250,000

©Institute for Clinical and Economic Review, 2022 Page E16
Evidence Report – Medications for Obesity Management Return to Table of Contents
Probabilistic Sensitivity Analysis
Probabilistic sensitivity analysis results are presented in the Report. Additional results, including
incremental cost-effectiveness scatterplots and acceptability curves are presented in Figure E4.
Figure E4. Results of Probabilistic Sensitivity Analysis, Incremental Cost-Effectiveness Scatterplots
and Acceptability Curve
Incremental Cost-Effectiveness Scatterplot
Y-axis: Incremental Cost (USD)
X-axis: Incremental Effectiveness (QALY Gained)
Acceptability Curve
Y-axis: Probability Cost Effective
X-axis: Cost-Effectiveness Threshold (USD/QALY)
Semaglutide v. Lifestyle Modif
ication
Liraglutide v. Lifestyle Modification
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
$400,000
-0.5 0 0.5 1 1.5 2
0%
20%
40%
60%
80%
100%
$0 $100,000 $200,000 $300,000
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
-0.2 0 0.2 0.4 0.6 0.8
Incremental Effectiveness (QALY gained)
0%
20%
40%
60%
80%
100%
$0 $100,000 $200,000 $300,000

©Institute for Clinical and Economic Review, 2022 Page E17
Evidence Report – Medications for Obesity Management Return to Table of Contents
Incremental Cost-Effectiveness Scatterplot
Y-axis: Incremental Cost (USD)
X-axis: Incremental Effectiveness (QALY Gained)
Acceptability Curve
Y-axis: Probability Cost Effective
X-axis: Cost-Effectiveness Threshold (USD/QALY)
Phentermine/Topiramate v. Lifestyle Modification
Naltrexone/Bupropion v. Lifestyle Modification
-$40,000
-$30,000
-$20,000
-$10,000
$0
$10,000
$20,000
$30,000
$40,000
-0.5 0 0.5 1
0%
20%
40%
60%
80%
100%
$0 $100,000 $200,000 $300,000
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
-0.2 0 0.2 0.4 0.6
0%
20%
40%
60%
80%
100%
$0 $100,000 $200,000 $300,000

©Institute for Clinical and Economic Review, 2022 Page E18
Evidence Report – Medications for Obesity Management Return to Table of Contents
Incremental Cost-Effectiveness Scatterplot
Y-axis: Incremental Cost (USD)
X-axis: Incremental Effectiveness (QALY Gained)
Acceptability Curve
Y-axis: Probability Cost Effective
X-axis: Cost-Effectiveness Threshold (USD/QALY)
Sema
glutide v. Phentermine/Topiramate
Semaglutide v. Bupropion/Naltrexone
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
-0.2 0 0.2 0.4 0.6 0.8
0%
20%
40%
60%
80%
100%
$0 $100,000 $200,000 $300,000
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
-0.5 0 0.5 1 1.5
0%
20%
40%
60%
80%
100%
$0 $100,000 $200,000 $300,000

©Institute for Clinical and Economic Review, 2022 Page E19
Evidence Report – Medications for Obesity Management Return to Table of Contents
E5. Scenario Analyses
Key scenario analysis results are presented in the Report. Indirect costs of each cardiovascular
conditions were calculated from published research and public data (Table E11). Additional results
for the societal perspective scenario analyses are presented by incremental cost per outcome
gained in Table E12. Changes to inputs for Comorbidity X scenarios are presented in Table E13
whereas cost per life year, QALY, and evLY gained results of the Comorbidity X scenarios are
presented in Tables E14 and E15, respectively. In scenario analyses, we explored how cost
effectiveness is impacted by the average BMI prior to initiating treatment and for a population of
patients with an equal male to female ratio. Cost per life year, QALY, and evLY gained results of the
class III obesity scenarios and similar male-female ratio scenario are presented in Tables E16-E18.
Table E11. Societal Perspective Indirect Cost* Inputs
Parameter
Input
Source
Indirect Cost of Type 2 Diabetes $3,245
American Diabetes
Association 2018
103
Indirect Cost of Myocardial Infarction Management $3,467
American Heart
Association/American
Stroke Association
158
Indirect Cost of Stroke Management $5,271
American Heart
Association/American
Stroke Association
158
Indirect Cost of Other Cardiovascular Conditions $7,340
American Heart
Association/American
Stroke Association
158
Indirect Cost of Heart Failure
$10,403
Cook 2014
108
*Annual productivity loss calculated from the ratio of direct vs. indirect burden of each chronic condition
management.
Table E12. Societal Perspective Incremental Cost-Effectiveness Ratios
Treatment Comparator
Cost per Life
Year Gained
Cost per QALY
Gained
Cost per
evLY Gained
Semaglutide
Lifestyle modification
$568,000
$217,000
$214,000
Liraglutide
Lifestyle modification
$1,149,000
$461,000
$451,000
Phentermine/Topiramate
Lifestyle modification
P/T less costly, more effective
Bupropion/Naltrexone
Lifestyle modification
$307,000
$106,000
$104,000
Semaglutide
Liraglutide
$34,000
$12,000
$12,000
Phentermine/topiramate
$1,068,000
$447,000
$443,000
Bupropion/naltrexone
$646,000
$254,000
$252,000
Liraglutide
Phentermine/topiramate $23,592,000
P/T less costly,
more effective
P/T less
costly, more
effective
Bupropion/naltrexone
$1,921,000
$908,000
$889,000
Phentermine/Topiramate
Bupropion/naltrexone
P/T less costly, more effective
evLY: equal-value life year, P/T: phentermine/topiramate, QALY: quality-adjusted life year, SEM: semaglutide

©Institute for Clinical and Economic Review, 2022 Page E20
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table E13. Inputs for Comorbidity X Scenarios
Parameter
Input
Source
Cancer Inputs
Annual Incidence of Cancer for Ages 40-49 years
0.28%
White 2014
159
Annual Incidence of Cancer for Ages 50-59 years
0.68%
Annual Incidence of Cancer for Ages 60-69 years
1.39%
Annual Incidence of Cancer for Ages 70-79 years
1.95%
Annual Incidence of Cancer for Ages ≥80 years
1.83%
Relative Risk of Cancer per One Unit Increase in BMI
1.04
Munsell 2014
160
Relative Risk of Death with Cancer
3.73
Kim 2022
105
Annual Cost of Cancer
$15,756
CKD Inputs
Annual Incidence of CKD for BMI Range 25-30
0.32%
Mohammedi 2018
161
Annual Incidence of CKD for BMI Range 30-35
0.37%
Annual Incidence of CKD for BMI Range 35-40
0.51%
Annual Incidence of CKD for BMI Range 40-45
0.79%
Relative Risk of Death with CKD
2.48
USRDS 2015
162
Annual Cost of CKD
$12,497
USRDS 2021
163
BMI: body mass index, CKD: chronic kidney disease
Table E14. Comorbidity X Scenario Analysis (Cancer)
Treatment Comparator
Cost per Life
Year Gained
Cost per QALY
Gained
Cost per
evLY Gained
Semaglutide
Lifestyle modification
$480,000
$215,000
$211,000
Liraglutide
Lifestyle modification
$976,000
$447,000
$434,000
Phentermine/Topiramate
Lifestyle modification
$14,000
$6,000
$6,000
Bupropion/Naltrexone
Lifestyle modification
$242,000
$106,000
$102,000
Semaglutide
Liraglutide
$65,000
$29,000
$28,000
Phentermine/topiramate
$968,000
$447,000
$441,000
Bupropion/naltrexone
$564,000
$255,000
$251,000
Liraglutide
Phentermine/topiramate
P/T less costly, more effective
Bupropion/naltrexone
$1,945,000
$953,000
$926,000
Phentermine/Topiramate
Bupropion/naltrexone
P/T less costly, more effective
BMI: body mass index, CKD: chronic kidney disease, P/T: phentermine/topiramate

©Institute for Clinical and Economic Review, 2022 Page E21
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table E15. Comorbidity X Scenario Analysis (Chronic Kidney Disease)
Treatment Comparator
Cost per Life
Year Gained
Cost per QALY
Gained
Cost per
evLY Gained
Semaglutide
Lifestyle modification
$504,000
$213,000
$209,000
Liraglutide
Lifestyle modification
$997,000
$439,000
$426,000
Phentermine/Topiramate
Lifestyle modification
$9,000
$4,000
$3,000
Bupropion/Naltrexone
Lifestyle modification
$242,000
$100,000
$97,000
Semaglutide
Liraglutide
$66,000
$27,000
$27,000
Phentermine/topiramate
$1,056,000
$460,000
$455,000
Bupropion/naltrexone
$601,000
$256,000
$252,000
Liraglutide
Phentermine/topiramate
P/T less costly, more effective
Bupropion/naltrexone
$2,003,000
$965,000
$939,000
Phentermine/Topiramate
Bupropion/naltrexone
P/T less costly, more effective
BMI: body mass index, CKD: chronic kidney disease, QALY: quality-adjusted life year
Table E16. Class III Obesity Scenario 1, Baseline BMI of 40-45 m
2
/kg (Average BMI of 42.5)
Treatment Comparator
Cost per Life
Year Gained
Cost per QALY
Gained
Cost per
evLY Gained
Semaglutide
Lifestyle modification
$557,000
$209,000
$205,000
Liraglutide
Lifestyle modification
$1,203,000
$464,000
$451,000
Phentermine/Topiramate
Lifestyle modification
$5,000
$2,000
$2,000
Bupropion/Naltrexone
Lifestyle modification
$334,000
$111,000
$108,000
Semaglutide
Liraglutide
$44,000
$16,000
$16,000
Phentermine/topiramate
$1,001,000
$415,000
$408,000
Bupropion/naltrexone
$620,000
$241,000
$237,000
Liraglutide
Phentermine/topiramate
P/T less costly, more effective
Bupropion/naltrexone
$2,059,000
$941,000
$913,000
Phentermine/Topiramate
Bupropion/naltrexone
P/T less costly, more effective
evLY: equal-value life year, P/T: phentermine/topiramate, QALY: quality-adjusted life year, SEM: semaglutide
Table E17. Class III Obesity Scenario 2, Baseline BMI of 45-50 m
2
/kg (Average BMI of 47.5)
Treatment Comparator
Cost per Life
Year Gained
Cost per QALY
Gained
Cost per
evLY Gained
Semaglutide
Lifestyle modification
$573,000
$205,000
$200,000
Liraglutide
Lifestyle modification
$1,414,000
$501,000
$486,000
Phentermine/Topiramate
Lifestyle modification
$11,000
$3,000
$3,000
Bupropion/Naltrexone
Lifestyle modification
$370,000
$115,000
$111,000
Semaglutide
Liraglutide
$25,000
$9,000
$9,000
Phentermine/topiramate
$1,014,000
$403,000
$394,000
Bupropion/naltrexone
$628,000
$234,000
$228,000
Liraglutide
Phentermine/topiramate
P/T less costly, more effective
Bupropion/naltrexone
$2,630,000
$1,118,000
$1,079,000
Phentermine/Topiramate
Bupropion/naltrexone
P/T less costly, more effective
evLY: equal-value life year, P/T: phentermine/topiramate, QALY: quality-adjusted life year, SEM: semaglutide

©Institute for Clinical and Economic Review, 2022 Page E22
Evidence Report – Medications for Obesity Management Return to Table of Contents
Table E18. Similar Proportion of Male and Female (50:50) Scenario
Treatment Comparator
Cost per Life
Year Gained
Cost per QALY
Gained
Cost per
evLY Gained
Semaglutide
Lifestyle modification
$535,000
$228,000
$225,000
Liraglutide
Lifestyle modification
$1,043,000
$466,000
$455,000
Phentermine/Topiramate
Lifestyle modification
$17,000
$7,000
$6,000
Bupropion/Naltrexone
Lifestyle modification
$296,000
$116,000
$114,000
Semaglutide
Liraglutide
$74,000
$30,000
$30,000
Phentermine/topiramate
$992,000
$457,000
$453,000
Bupropion/naltrexone
$609,000
$267,000
$264,000
Liraglutide
Phentermine/topiramate
$70,143,000
P/T less costly, more effective
Bupropion/naltrexone
$1,781,000
$917,000
$896,000
Phentermine/Topiramate
Bupropion/naltrexone
P/T less costly, more effective
evLY: equal-value life year, P/T: phentermine/topiramate, QALY: quality-adjusted life year, SEM: semaglutide
E6. Heterogeneity and Subgroups
There are patient or cohort-specific factors that may affect treatment response in patients with
overweight or obesity. Our model was not specifically designed to test the cost effectiveness of
weight-management in patients with diabetes mellitus.
We explored how the cost effectiveness is impacted by the average BMI prior to initiating
treatment and male to female ratio. Incremental cost-effectiveness ratios for the patients with
class III obesity and population consisting of similar proportion of male and female are presented in
Table E19.
Table E19. Analysis to Address Potential Heterogeneity Effect Across Subpopulations: Class III
Obesity or Similar Male and Female Proportions (50:50), Incremental Cost-Effectiveness (QALY)
Ratios
Treatment Comparator
BMI 40-45 m
2
/kg
(Average: 42.5)
BMI 45-50 m
2
/kg
(Average: 47.5)
Male:
Female
50:50
Semaglutide
Lifestyle modification
$209,000
$205,000
$228,000
Liraglutide
Lifestyle modification
$464,000
$501,000
$466,000
Phentermine/Topiramate
Lifestyle modification
$2,000
$3,000
$7,000
Buproprion/Naltrexone
Lifestyle modification
$111,000
$115,000
$116,000
Semaglutide
Liraglutide
$16,000
$9,000
$30,000
Phentermine/topiramate
$415,000
$403,000
$457,000
Buproprion/naltrexone
$241,000
$234,000
$267,000
Liraglutide
Phentermine/topiramate
Phentermine/topiramate less costly, more effective
Buproprion/naltrexone
$941,000
$1,118,000
$917,000
Phentermine/Topiramate
Buproprion/naltrexone
Phentermine/topiramate less costly, more effective
BMI: body mass index

©Institute for Clinical and Economic Review, 2022 Page E23
Evidence Report – Medications for Obesity Management Return to Table of Contents
E7. Prior Economic Models
Our study adapted structurally-advanced prior economic models that focused on causal
associations between BMI and cardiovascular comorbidities. Borisenko et al. developed a bariatric
surgery Markov model in which the natural course of weight-related cardiovascular conditions was
included as separate Markov states.
90,91,164-166
A recently developed model linked BMI and glucose
intolerance with the onset of diabetes mellitus and cardiovascular complications.
167
Similar to our
model, both models incorporated the Framingham risk equation as a predictor of cardiovascular
comorbidity onset. Due to ongoing uncertainty around the causal association between weight loss
and non-cardiovascular comorbidities, the bariatric surgery Markov model excluded cancer,
osteoarthritis, sleep apnea, and chronic kidney disease. In our model, we tested the potential
influence of the non-cardiovascular conditions on the cost effectiveness using an add-on
Comorbidity X state. This structural adaptation to the model, with the inclusion of conditions not
evaluated in the base case, could be considered as an advanced method of scenario analysis in
situations with limited evidence regarding exposure-outcome association.
Additionally, we critically evaluated economic models involving GLP-1 receptor agonists in the US
health care setting. Lee at al. analyzed the cost effectiveness of medication-assisted weight loss
options using treatment cost and BMI-dependent quality of life without including comorbid states
in the model.
168
Similar to our findings, this study concluded that 1) phentermine/topiramate was
the most cost-effective strategy; 2) patients on semaglutide gained the largest clinical and QALY
benefits; 3) liraglutide was dominated by phentermine/topiramate and semaglutide. These
conclusions regarding semaglutide and liraglutide were supported by a recent analysis of four GLP-1
receptor agonists.
169
A more detailed comparison of findings could not be made because the
structure of the two previous models notably differed from our model.
Another recent publication analyzed the cost effectiveness of medication-assisted weight loss
treatment strategies compared to lifestyle modification.
105
The study adapted a model to evaluate
the cost effectiveness of semaglutide 2.4 mg for the treatment of adult patients with overweight or
obesity. The Markov model examined semaglutide compared to no treatment, diet and exercise
alone, and standard-of-care therapy options (liraglutide 3 mg, phentermine/topiramate, and
bupropion/naltrexone) from the US third-party payer’s perspective over a 30-year time horizon.
Treatment duration with any therapy (aside from diet and exercise) did not exceed two years, after
which a gradual weight regain to baseline was applied to address natural weight gain until the end
of the time horizon. In the model, patients could transition between no comorbidity, single
comorbidity, dual comorbidity, multi-comorbidity, and death. Comorbidities included in the model
were post-myocardial infarction, type 2 diabetes mellitus, post-stroke, obstructive sleep apnea, and
cancer. Patients could experience acute events of bariatric surgery, acute coronary syndrome,
stroke/transient ischemic attack, and knee replacements. In this study, the base-case incremental
cost-effectiveness ratios (cost per QALY) from this model for semaglutide 2.4 mg compared to

©Institute for Clinical and Economic Review, 2022 Page E24
Evidence Report – Medications for Obesity Management Return to Table of Contents
liraglutide 3 mg, phentermine/topiramate, bupropion/naltrexone, diet and exercise, and no
treatment were $23,556, $144,296, $127,518, $122,549, and $27,113, respectively. Liraglutide 3
mg, phentermine/topiramate, and bupropion/naltrexone compared to diet and exercise resulted in
incremental cost-effectiveness ratios of $439,200, $32,700, and $86,500. In an exercise assessing
how our model results compared with those of this published model, we edited our model to
include a two-year treatment, 30-year time horizon, and used disutilities for cardiovascular events
and diabetes mellitus reported in this study.
105
The resulting incremental cost-effectiveness ratio
estimates for semaglutide compared with lifestyle modification from our model were
approximately $10,000 per QALY gained less than the same comparison reported by Kim N et al.
This remaining difference is explained by structural differences, higher mortality leading to lower
QALY gains, and other differences in inputs not modeled in our validation exercise. Due to concerns
associated with attributing long-term benefits to a short-term (i.e., two-year) treatment and the
likely poor performance of the ACC/AHA models in predicting cardiovascular risk after
discontinuation of short-term treatment as well as the potential risks of weight cycling, we chose to
focus solely on evaluating the cost effectiveness of lifetime treatment.
170,171
Additional differences noted between these two models included the incorporation of certain
cancers, sleep apnea, and the acute events of bariatric surgery and knee replacements.
105
We
evaluated the potential impact of cancers and chronic kidney disease in scenario analyses. In our
Comorbidity X scenarios, we determined that conditions other than cardiovascular conditions likely
have a nominal impact on incremental cost-effectiveness ratios. Additionally, we were unable to
assess differences in the application of risk equations to models. For example, Kim et al. utilized
Framingham Recurring Coronary Heart Disease and United Kingdom Prospective Diabetes Study risk
equations within their model structure, whereas we used the ACC/AHA risk equation model, which
incorporates updated estimates from Framingham but not changes in cardiovascular risk due to
HbA1C. Finally, treatment efficacy inputs were derived directly from clinical trials in this published
analysis, whereas our analysis involved conducting an NMA to derive the primary effectiveness
inputs.

©Institute for Clinical and Economic Review, 2022 Page E25
Evidence Report – Medications for Obesity Management Return to Table of Contents
F. Potential Budget Impact: Supplemental
Information
Methods
The primary aim of the potential budgetary impact analysis is to document the percentage of
patients who could be treated at selected semaglutide prices without crossing a potential budget
impact threshold that is aligned with overall growth in the US economy. For 2022-2023, the five-
year annualized potential budget impact threshold that should trigger policy actions to manage
access and affordability is calculated to be approximately $777 million per year
for a novel
prescription drug therapy.
Potential budget impact was defined as the total differential cost of using semaglutide rather than
relevant existing therapy (alone) for the treated population, calculated as differential health care
costs (including drug costs) minus any offsets in these costs (for instance, due to offsets in major
adverse cardiovascular events). All costs were undiscounted and estimated over one- and five-year-
time horizons. The five-year timeframe was of primary interest, given the potential for cost offsets
to accrue over time and to allow a more realistic impact on the number of patients treated with the
new therapy. This longer-term budget impact horizon of five years is aligned with the durable
treatment persistence assumption key to our underlying cost-effectiveness analytic approach.
To estimate the size of the potential candidate populations for treatment, we use the US adult
population size and prevalence of obesity and overweight in conjunction specific weight-related
comorbidities or biomarkers for such. Specifically, we utilize deidentified and merged patient
records from the National Health and Nutrition Examination Survey (NHANES) over the 2017-2018
and 2019-March 2020 data collection cycles for estimates of prevalence.
NHANES is a program
combining interviews and physical examinations to assess health and nutritional status among US
adults and children.
To determine size of the salient cohort with overweight and with weight-
related comorbidities specifically, we use the following patient-level data as captured within
NHANES, where patient records must have evidence of one or more of the following in addition to
reporting with overweight (defined as 27.0 kg/m
2
≤BMI<30 kg/m
2
): 1) Ever told you have high blood
pressure, 2) Ever told you have high cholesterol, 3) Ever told you have prediabetes, 4) HbA1C ≥6.5%,
5) Ever told you have diabetes, 6) Insulin level ≥23 microunits/mL, and 7) Stop breathing three or
more nights a week. Accordingly, we estimate a combined prevalence value for US adults with BMI
≥30 or 27.0 kg/m
2
≤BMI<30 kg/m
2
with one or more weight-related comorbidities at 53.53% (41.96%
with obesity, 11.57% with overweight and one or more weight-related comorbidities). Semaglutide
captures market share proportionally from all modeled comparators (liraglutide,
phentermine/topiramate, bupropion/naltrexone, lifestyle modification alone), with semaglutide

©Institute for Clinical and Economic Review, 2022 Page E26
Evidence Report – Medications for Obesity Management Return to Table of Contents
achieving 100% market share by year five. This is a key modeling assumption aimed at
understanding the proportion of the total population that can be treated without crossing the
annual budget impact threshold.
Results
Table F1 describes the per-patient budget impact calculations in more detail, based on WAC
($17,597.48 per year), discounted WAC ($13,618.22 per year), and the prices to reach $150,000,
$100,000, and $50,000 per QALY ($9,700, $7,500, and $5,300 per year, respectively) compared
lifestyle modification alone. Similarly, Figure F1 visualizes semaglutide’s cumulative net budget
impact per treated patient per year at its calculated net price, assuming an incremental 20% uptake
per year.
Table F1. Per-Patient Budget Impact Calculations Over a Five-Year Time Horizon
Average Annual Per Patient Budget Impact
WAC
Discounted
WAC
$150,000/QALY $100,000/QALY $50,000/QALY
Semaglutide
$13,300
$9,400
$5,700
$3,500
$1,400
QALY: quality-adjusted life year, WAC: wholesale acquisition cost
Figure F1. Cumulative Per-Patient Budget Impact Calculations Over a Five-Year Time Horizon at
Semaglutide Net Price
$9,700
$19,300
$28,700
$37,900
$47,000
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
$35,000
$40,000
$45,000
$50,000
Year 1 Year 2 Year 3 Year 4 Year 5
Cumulative Annual Budget Impact Per
Treated Patient
